Shared Attributes of Responsibility and Emotion in Patients With Lung Cancer and Family Caregivers
Objectives: To compare the attributions and emotions held by patients with lung cancer (affected individuals) and family caregivers in their management of the disease.
Sample & Setting: A secondary data analysis of 304 affected individuals and 304 family caregivers. Participants were selected from five oncology outpatient settings.
Methods & Variables: Comparative analysis and regression modeling. Variables include responsibility, anger, and pride in managing lung cancer.
Results: Affected individuals reported higher self-oriented blame, fault, and anger than did family caregivers. Family caregivers reported more blame, fault, and anger toward the affected individual than toward themselves. Current smoking behavior of either the affected individual or family caregiver was associated with increased reports of self-oriented blame, fault, and anger. Additional research is needed to understand the attributional and emotional responses affected by the type of lung cancer, gender differences, and characteristics of the caregiving dyad.
Implications for Nursing: Nurses should be aware of the potential for affected individuals to experience internal (self) and external (family caregiver) sources of blame, fault, and anger. Knowledge of the reasons for current smoking behavior is important for understanding emotional responses and determining interventions.
Jump to a section
Lung cancer is a global concern, being cited as the most common cancer worldwide and accounting for 13% of the total number of new cancer cases diagnosed in 2012 (American Cancer Society, 2015; Ferlay et al., 2013). Despite decreasing trends in mortality and incidence, lung cancer still accounts for the largest number of deaths attributed to cancer (American Cancer Society, 2016; Canadian Cancer Society’s Advisory Committee on Cancer Statistics, 2015).
These trends and statistics are noteworthy from a nursing perspective because patients (i.e., affected individuals) with lung cancer tend to experience higher levels of psychological distress and symptom burden and lower quality of life compared to patients with other types of cancer (Lehto, 2014). Personal reactions to lung cancer, such as guilt, self-blame, self-deprecation, regret, and anger (Lehto, 2014) have been found to persist throughout the illness journey (Akechi et al., 2006).
A diagnosis of lung cancer also has a significant impact on the quality of life and psychological well-being of the family unit, particularly the primary family caregiver (FC) (Sarna et al., 2006). Recognized FC emotional reactions to lung cancer include both negative attributes (e.g., uncertainty or fear about the future, anger and blame toward self and/or the affected individual) and positive attributes (e.g., hope for recovery, pride in the affected individual’s efforts to manage the disease) (Kendall et al., 2015; Lobchuk, McClement, McPherson, & Cheang, 2012; Mosher, Jaynes, Hanna, & Ostroff, 2013).
Theoretical Framework
Weiner’s (1995) attribution theory provided the theoretical foundation for the preliminary and larger studies (Lobchuk et al., 2008, 2012) and this subsequent analysis. Attribution theory is focused on an individual’s beliefs or attributions about the cause and/or control of an outcome or another person’s behavior and is situated within a motivational cognitive emotional behavior sequence. According to attribution theory, an individual’s attempts to understand or explain the occurrence of a significant outcome gives rise to an emotional response, which ultimately influences behavior in a situation (e.g., helping or aggressive behavior) (Rudolph, Roesch, Gritemeyer, & Weiner, 2004).
Using Weiner’s (1995) attributional model and terminology as a framework, as affected individuals with lung cancer and their FCs engage in a cognitive process to explain and understand the ongoing management or progression of the disease, judgments or attributions of responsibility are made toward oneself or another. The outcome of these attributions can result in either positive emotional responses, such as pride and hopefulness, or a negative reaction, such as anger, which then affects outward behavior (Rudolph et al., 2004). As an illustration, if an affected individual engages in behaviors that are perceived by self or another to negatively affects the ongoing management of the lung cancer (e.g., the affected individual chooses not to follow treatment or lifestyle change recommendations), this may cause either the affected individual or the FC to attribute more responsibility to that person. According to Weiner’s theory, this could manifest in an emotional response of more anger and less pride felt toward self or the other person and negatively affect behavior in the form of reduced helping actions or outward antagonism. Therefore, for the purposes of this analysis, attribution theory was used to guide the selection of attributional and emotional reactions for comparison between affected individual and FC perspectives.
Methods
The secondary data analysis plan was designed to engage in a comparative analysis of data collected from 608 participants (or 304 dyads of affected individuals and FCs) on their attributional and emotional responses toward their ongoing management of lung cancer. Multiple regression was used to determine if demographic and caregiving relationship attributes had an influence on affected individuals’ and FCs’ attributional and emotional responses. Factor analysis was employed initially to examine the ability to aggregate questions into composite scores for the measures relative to the main research variables.
Sample
The dataset examined originates from the completed cross-sectional study in which Lobchuk et al. (2012) examined the impact of affected individuals’ smoking behavior on FC judgments of responsibility, emotional responses, and empathic helping behavior. After receiving ethical approval from the University of Manitoba Research Ethics Board and informed consent, affected individuals and their primary FCs were recruited by convenience sampling from five outpatient cancer care clinics in Winnipeg, Manitoba, Canada. Data collection occurred from September 2005 to February 2009 and involved participant completion of self-report questionnaires and rating scales. Affected individuals were medically diagnosed with any stage of lung cancer; aged 18 years or older; able to converse, read, and write in English; and demonstrated no evidence of mental confusion (i.e., score of 24 or greater out of 30 on the Mini-Mental State Exam [Folstein, Folstein, & McHugh, 1975]). Adult FCs were primarily involved in the care of the affected individual in their home setting, and able to converse, read, and write in English. The details of the study procedures are described elsewhere (Lobchuk et al., 2012).
Measures
In the preliminary analysis (Lobchuk et al., 2008) and the completed research (Lobchuk et al., 2012), the main research variables of responsibility, anger, and pride that form the foundational concepts (latent variables) in Weiner’s (1995) attribution model were represented by observed indicators used to measure the abstract constructs. For example, responsibility is a latent variable that was represented by the indicators of blame, fault, and responsibility. The construct of anger was measured through questions pertaining to anger, annoyance, and aggravation. Lastly, pride was represented by indicators of pride, satisfaction, and hopefulness (see Figure 1).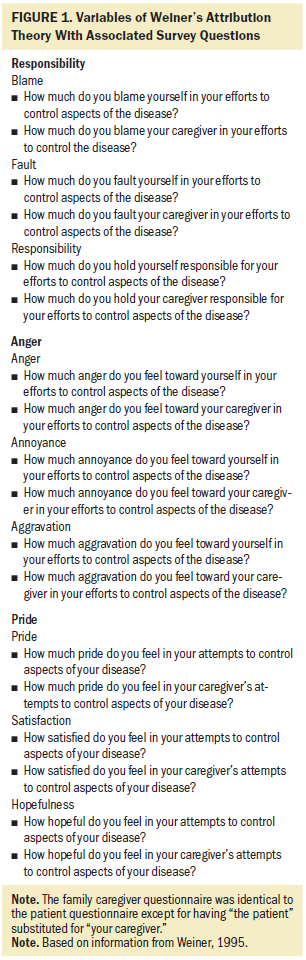
Because a standardized tool to measure these three constructs did not exist, the investigators created a series of questions that incorporated these indicators. The main research variables of responsibility, anger, and pride ascribed toward self or the other with respect to management of the disease were each measured by three sub-items, or indicators (respective to responsibility, anger, and pride), in the form of five-point Likert-type scales ranging from 0 (none) to 4 (entirely/a great deal) (Lobchuk et al., 2012). These questions were included with an investigator-developed tool that gathered demographic, smoking behavior, and caregiving relationship information via independent self-reports of affected individuals and FCs.
Data Analysis
The data analysis plan involved three main procedures: (a) a factor analysis of the indicators pertaining to the main research variables of responsibility, anger, and pride as a preliminary step to facilitate the analyses of the primary and secondary study objectives; (b) a comparative analysis of differences in responsibility, anger, and pride scores between affected individuals and FCs; and (c) regression modeling to test for relationships between the main research variables and individual demographic and caregiving relationship characteristics. Data analyses were performed using SAS®, version 9.4.
The initial step of the data analysis involved an examination of the indicators (observed variables) in relation to the latent variables of responsibility, anger, and pride. This was accomplished by calculating reliability estimates for these three variables using Cronbach alpha and by conducting a factor analysis using a principal component analysis with a varimax rotation method (Fabrigar, Wegener, MacCallum, & Strahan, 1999). The rationale for conducting a factor analysis was twofold. First, factor analysis on the FC data was undertaken in the preliminary analysis (Lobchuk et al., 2008) and completed research on the fulsome sample (Lobchuk et al., 2012) to examine the indicators (observed variables) relative to responsibility, anger, and pride. The results indicated congruence between the indicator and corresponding latent variables; therefore, factor analysis was conducted in this study to compare findings. The factor loadings for the FC data were similar to the results of Lobchuk et al. (2008, 2012), suggesting theoretical congruence between the measures and the latent variables.
Second, to facilitate comparison of the attributional and emotional responses between the affected individual and FC groups, the data needed to be examined for the ability to aggregate the six individual sub-items/questions for responsibility, anger, and pride into composite scores for each group. The indicators for responsibility, anger, and pride for both groups had Cronbach alpha values greater than 0.8 (with the exception of the affected individual responsibility value of 0.637), suggesting a high level of reliability between the individual indicators. Examination of the indicator factor loadings suggested that the scores could be aggregated as outlined in Table 1, resulting in newly created variables to allow comparison between the two groups. As an example, in consideration of the affected individuals’ responsibility scores, self-blame and self-fault in ongoing management of lung cancer loaded into one component (affected individual self-oriented responsibility), blame and fault toward the FC loaded into a second component (affected individual other-oriented responsibility), and holding both self and the FC responsible loaded into a third (affected individual shared responsibility).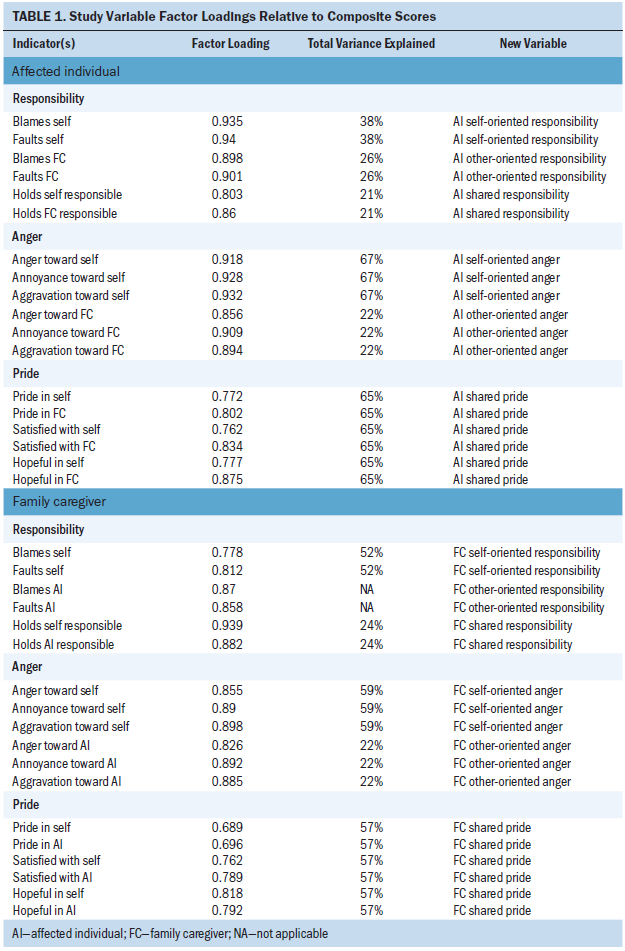
Overall, the indicator factor loadings aligned well between both groups, enabling the formation of six composite outcome variables of interest for both the affected individual and FC groups. All indicators of the pride variable were highly correlated, resulting in one combined variable (shared pride). The items that loaded into the two combined variables for anger represented an alignment in respect to internally (self-oriented anger) and externally (other-oriented anger) directed responses of anger in relation to managing the illness. For responsibility, the two indicators in relation to holding self and the other responsible for the ongoing management of the disease loaded into one component for both groups, resulting in the combined variable of shared responsibility. However, the four indicators representing attributions of blame and fault toward self and the other loaded into two components for affected individuals and one component for FCs. To address the incongruent loading of these indicators between the two groups, two combined variables were created based on the affected individuals’ responsibility results because these four indicators all correlated for the FC data. This resulted in the formation of the self-oriented responsibility and other-oriented responsibility variables.
The first study objective was to compare the attributional (responsibility) and emotional (anger and pride) responses of participants toward their respective management of the disease. The affected individuals and FCs were considered independent (non-paired) groups for this aspect of the analysis. Prior work by Zhang and Siminoff (2003) indicates affected individuals’ and FCs’ emotional responses to the experience would be personal and independent from the other’s perspective. Previous study findings on family communication indicated a desire by affected individuals and their FCs to avoid emotional distress, protect the other from harm or upset, and promote positive thinking, which may prevent an affected individual and their FC from discussing emotions and concerns with each other (Zhang & Siminoff, 2003). Pearson’s correlation and nonparametric (Mann-Whitney U) tests were employed.
The second study objective, to determine if certain demographic factors had an influence on affected individuals’ and FCs’ attributional and emotional responses, was addressed by conducting regression analyses. The effects of age, gender, type of lung cancer, level of education, current smoking behavior, and type and length of the FC relationship on participants’ responsibility and anger scores were analyzed using logistic regression models because assumptions relating to the normal distribution of residuals were not met for the responsibility and anger scores. To obtain binary scores for both responsibility and anger variables, scores of 0 were coded to represent no responsibility/anger, and any other score was collapsed to represent any degree of responsibility/anger. Participants’ pride scores were analyzed using a linear regression model as assumptions of normal distribution were met. Three independent variables in the regression models were recoded into binominal variables: level of education (less than high school; high school or greater), current smoking status (not currently smoking; currently smoking), and type of FC relationship (not spouse; spouse).
Results from the separate regression analyses for the affected individuals and FCs were similar in terms of interpretation of individual coefficients for the independent variables. Therefore, to simplify explanation of the findings, the affected individual and FC data were combined in the regression models and the results reported collectively.
Results
Demographics
Table 2 provides demographic information for the sample. Affected individuals with lung cancer (N = 304) had a mean age of 65 years (SD = 9.51; range = 40–105) and a majority were female (51%) and married (71%). Fifty-nine percent reported high school or higher level of education and 22% of affected individuals were smoking cigarettes to some extent at the time of the study. FCs (N = 304) had a mean age of 59 years (SD = 12.7; range = 20–84) and a majority were female (66%) and married (81%). Sixty-eight percent had achieved high school or higher level of education and 22% currently smoked cigarettes to some extent at the time of the study. In relation to caregiving information, 66% of the FCs were the affected individual’s spouse and 75% of the caregivers lived with the affected individual.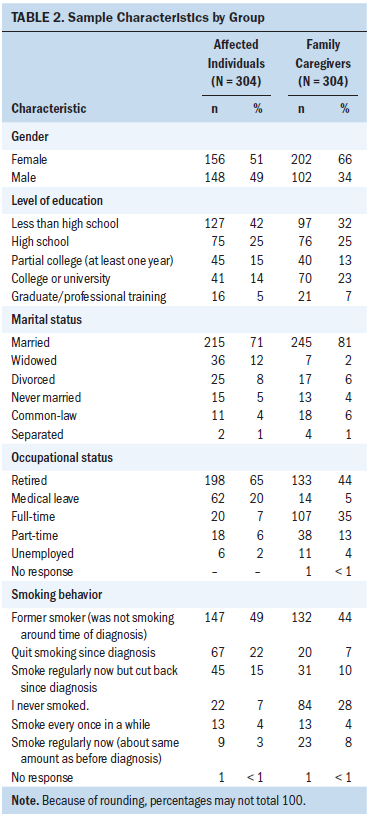
Regarding affected individuals’ available lung cancer diagnostic information, 78% (n = 238) had NSCLC and 21% (n = 64) had SCLC. Of those with NSCLC, 64% had stage III or IV cancer, and 44% of affected individuals with SCLC reported extensive involvement of the disease. Forty-nine percent of the affected individuals with lung cancer were receiving active treatment at the time of the survey. FCs were most frequently a spouse (66%) or son/daughter (16%). The most commonly reported length of caregiving relationship was from 0-9 months (49%), with a timeframe of greater than 36 months being the second most common (29%) response. Seventy-two percent of the FCs reported that they frequently or always assisted the affected individual in coping with his or her medical condition and symptoms.
Affected Individual and Family Caregiver Attributional and Emotional Responses
Descriptive statistics and comparative results for the combined responsibility, anger, and pride scores in relation to management of the disease are provided in Table 3. To address the first objective, affected individuals had significantly higher average scores on the self-oriented responsibility questions compared to FCs’ self-oriented responsibility scores. However, FCs had significantly higher average scores on other-oriented responsibility questions compared to affected individuals. For the self-oriented anger scores, affected individuals reported significantly higher feelings of anger, annoyance, and aggravation toward themselves compared to FCs. Conversely, FCs reported slightly higher scores compared to affected individuals for the other-oriented anger questions, which addressed anger, annoyance, and aggravation toward the affected individual. FCs had slightly higher scores for shared pride compared to affected individuals; however, the difference was not significant. Regarding correlations in responsibility and emotional scores, significant but weak positive correlations were noted between affected individual and FC responses on the other-oriented responsibility (r = 0.136, p < 0.05), self-oriented anger (r = 0.175, p < 0.01), and shared pride (r = 0.339, p < 0.01) scores.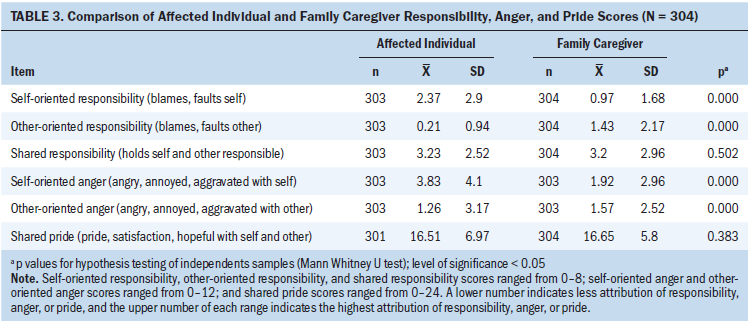
Effects of Variables on Attributional and Emotional Responses
In consideration of the second study objective, the results of the logistic regression analysis of the responsibility and anger variables are presented in Table 4. Significant findings were noted in relation to the odds ratios (ORs) for the three responsibility measures and the self-oriented anger measure. For self-oriented responsibility, the model associated reports of self-directed blame and fault with current smoking (OR = 2.43, 95% CI [1.54, 3.83]) and male gender (OR = 1.52, 95% CI [1.03, 2.26]). If a diagnosis of NSCLC was present, the model suggested less odds of reporting self-blame and fault (OR = 0.63, 95% CI [0.34, 0.99]). The results indicated less chance of reporting blame and fault toward the other person (other-oriented responsibility) with increasing age (OR = 0.54, 95% CI [0.32, 0.93]) and when the affected individual had NSCLC (OR = 0.59, 95% CI [0.37, 0.92]). Finally, in relation to the responsibility variable, the analysis supported a relationship between reports of increased shared responsibility if the length of the caregiving relationship was within a 10- to 18-month timeframe (OR = 2.18, 95% CI [1.05, 4.52]) and with higher levels of education (OR = 1.62, 95% CI [1.1, 2.39]). Only one significant finding was noted in relation to the anger variables. The model suggested a relationship between current smoking and self-directed anger, annoyance, and aggravation (OR = 1.84, 95% CI [1.21, 2.8]).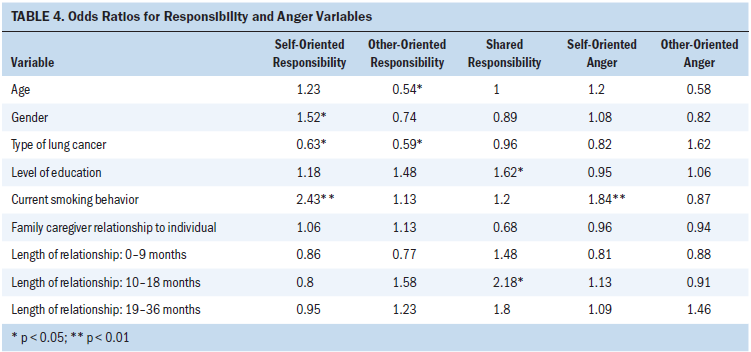
Regarding the linear regression analysis of pride (not reported in Table 4), the model explained 6.5% of the variance in the pride scores (F = 5.1, df = 8, p < 0.000). Results of the regression suggested that lower ratings of pride would be reported by affected individuals who currently smoke (beta = –1.26, 95% CI [–2.49, –0.03], p = 0.04) and if the affected individual has NSCLC (beta = –1.31, 95% CI [–2.56, –0.06], p = 0.04). If the FC was the affected individual’s spouse, the model suggested higher ratings of pride (beta = 2.79, 95% CI [1.64, 3.93], p < 0.000).
Discussion
As guided by Weiner’s (1995) attributional theory, the primary study objective was to compare attributional perspectives and emotional responses of affected individuals and FCs in respect to the management of lung cancer. Affected individuals tended to blame and fault themselves more so than FCs. FCs also tended to blame and fault the affected individuals more regarding responsibility in managing the disease; affected individuals blamed and faulted FCs less. Similarly, affected individuals reported more anger, annoyance, and aggravation directed toward self than at FCs. On the other hand, FCs indicated greater responses of anger, annoyance, and aggravation toward affected individuals than affected individuals did toward FCs. Results from this analysis support the preliminary findings by Lobchuk et al. (2008) where affected individuals reported significantly more self-directed responsibility and anger, but less toward the FC. Conversely, they too found that FCs attributed more blame, fault, and responsibility toward affected individuals than toward themselves.
Comparative analyses of affected individuals and FC pride scores produced interesting but unexpected results. No significant difference existed between pride scores that were moderately high. These findings suggest that, although there appeared to be some negative emotional responses in relation to responsibility and anger directed toward the affected individual, these responses did not appear to adversely affect the sense of pride, satisfaction, and hopefulness that the affected individual and the FC felt in relation to managing the disease. Although literature cites the existence and persistence of anger, self-blame, fear, and uncertainty within the context of a lung cancer diagnosis, evidence shows that positive emotions, such as hope for recovery, coexist (Kendall et al., 2015). Dealing with lung cancer represents the complex coexistence of negative and positive emotional responses that invokes a flexible nursing approach to mitigate potential adverse outcomes while drawing on emotional strengths, such as hope and pride.
The secondary objective of the study was to determine if demographic and caregiving relationship factors were related to attributional and emotional responses of participants. The relationship between current smoking behavior and increased self-oriented ascriptions of blame, fault, and anger, and decreased pride is a notable finding. Although causality cannot be established with this one-time convenience sample, bi-directional relationships can be considered. From one perspective, if affected individuals blame themselves and hold the belief that their smoking behavior was the cause of the lung cancer (Weiss et al., 2016), attributions of self-directed blame and fault may transfer into their ongoing efforts to manage the disease, particularly if they continue to smoke. The resultant emotional reactions of anger and lessened pride may have a negative impact on the person’s overall emotional state and quality of life. However, a second perspective stems from the strong connection that has been established between anger, stress, and smoking. In affected individuals who smoke, smoking behavior tends to increase in response to stress or negative affect, such as anger, anxiety, or guilt, with the expectation that it will help alleviate these mood states (Kassel, Stroud, & Paronis, 2003). Therefore, it follows that, if an individual is experiencing self-oriented blame, fault, and anger within the context of a lung cancer diagnosis, they may continue to smoke as a coping mechanism to help manage their stress and negative affect.
Another finding of interest is the association between a diagnosis of NSCLC and lower reports of ascribed self- and other-oriented blame and fault, and lower feelings of pride; this relationship has not yet been documented in the literature to the best of the authors’ knowledge. It is plausible that not all individuals believed smoking caused their lung cancer (regardless of type of lung cancer) (Lehto, 2007). This could explain why attributions of responsibility directed toward the self or other as to the cause or ongoing management of this form of lung cancer may not be experienced by some affected individuals. Aggressiveness, rapidity of spread, and survival rates also differ between the different types of NSCLC (American Cancer Society, 2016), which can mitigate an affected individual’s or FC’s ascriptions of responsibility and emotional responses. Because the data collected in the original study (Lobchuk et al., 2012) did not identify the type of NSCLC (i.e., adenocarcinoma, squamous cell carcinoma, or large cell carcinoma), it is difficult to draw inferences from the data. Additional research is needed to investigate the existence and underlying causes of the relationship between the type and stage of lung cancer and ascriptions of blame and fault toward self and the other in the caregiving dyad.
Also of interest to nurses is the relationship between increased reports of self-oriented blame and fault and male gender. This supports previously reported outcomes by Weiss et al. (2016), who also found an association between male gender and higher reports of self-blame in lung cancer. Although the reason for this relationship cannot be firmly established from those data, it is plausible that this result may be related to gender roles and socialized responses to illness that warrant additional research.
The association between higher levels of education and increased shared responsibility in managing the disease might be explained by mutual knowledge-seeking expectations and behaviors in response to the ongoing management of the illness. This may be a factor for the nurse to identify and consider in relation to the acceptance and provision of teaching and health information to support the dyad in their ongoing efforts to manage the condition.
Regarding aspects of the caregiving relationship, the findings suggestive of a relationship between a 10- to 18-month caregiving relationship and higher reports of shared responsibility also are of significance to nurses. Because one-year lung cancer survival rates are cited as 44% (American Cancer Society, 2016), affected individuals and their FCs in long-term relationships need to be jointly supported in their shared responsibility to manage the condition up to and beyond expectations for survival. Related to this finding, another association was found between increased reports of pride and spousal caregivers. Assuming that affected individuals would be living with their spouse, it is plausible that this finding is because the dyad would spend more consistent time together, allowing more opportunity to observe and appreciate efforts made toward managing the illness. Because these findings have not been identified in previous research, the characteristics of the caregiving relationship represent another potential area for further development.
Limitations
Major limitations are related to the convenience sample and use of self-report data collection methods on the sensitive topic of judgments of responsibility and emotional responses in the context of a dire and stigmatized cancer diagnosis. In addition, the study was cross-sectional in nature because data were collected at only one time point, which does not allow for causal inferences or further investigation on changes in attributional and emotional responses throughout the cancer journey. The sample of affected individuals was obtained at urban clinic settings, which makes it difficult to generalize the findings to rural settings. In addition, this sample was comprised mainly of English-speaking and married individuals from middle-income families; this also limits study generalizability. Information collected on the type and amount of assistance (i.e., physical and/or emotional) needed by the affected individuals with lung cancer and provided by FCs is somewhat limited within the dataset. These factors could affect the FCs’ psychological and emotional responses to the situation, specifically considering that 48% of the FCs in this sample reported working full- or part-time.
Lastly, a standardized and validated tool was not employed to measure the main research variables of responsibility, anger, and pride. Regardless, most sub-items correlated well to each other and loaded acceptably into the factor analysis, enabling the creation of component scores.
Implications for Nursing
Affected individuals and FCs dealing with lung cancer need ongoing support from a variety of sources throughout their illness journey (Luszczynska, Pawlowska, Cieslak, Knoll, & Scholz, 2013; Mosher et al., 2013). Nurses must attend to the psychosocial and emotional needs of affected individuals and their FCs as a necessary component of person- and family-centred care. This analysis offers clarity related to what attributional and emotional responses the nurse can expect to deal with when providing support to affected individuals and their FCs.
Based on the outcomes of this study, nurses should be aware that affected individuals and their FCs can express a complex mix of negative attributes (judgments of blame and fault) toward the affected individual while, at the same time, report a degree of pride in their shared efforts to manage the illness. In addition, the nurse should appreciate that the affected individual may experience blame, fault, and anger reactions from both internal (self) and external (FC) sources. The experience of anger is particularly concerning from a nursing perspective, as anger has been found to persist throughout the lung cancer experience (Akechi et al., 2006). This, in turn, can affect quality of life for both the affected individual and the FC (Sarna et al., 2006).
From the FC perspective, previous research has suggested that the lung cancer experience for FCs involves attending to the affected individual’s emotional needs as well as their own needs (Mosher et al., 2013). This study’s findings suggest that nurses need to be aware of the potential for the FC to ascribe fault and blame to the affected individual with lung cancer and the resultant emotional reactions (i.e., anger or guilt) that may negatively influence the FC’s emotional and physical support (Lobchuk et al., 2012).
To intervene effectively in these situations, the nurse should first consider and assess for the existence of self- or other-directed blame, fault, and anger within the FC dyad. If these ascriptions of responsibility and emotional responses are present, it would be important for the nurse to explore and understand the “why” behind these reactions to help inform the intervention. Subsequent action could entail drawing on sources of positive emotional responses, such as pride and hopefulness, to counterbalance affected individuals’ and FCs’ negative emotional reactions throughout the illness experience. In addition, the nurse may need to consider and discuss amenable options for emotional and psychological support in the form of individual or dyad counseling or even a group therapy intervention.
A final consideration for nursing practice is related to the implications of current smoking behavior of either the person or FC (i.e., 22% of both the affected individuals and FCs currently smoked at the time of this study). The study findings indicated that if either the affected individual or FC currently smoked, they ascribed more blame and fault and reported more anger toward self in the context of managing the disease. Ascriptions of responsibility such as self-blame can potentially have negative effects on a person’s psychological and emotional state; however, conversely, it also can motivate positive behavioral changes, such as smoking cessation (Weiner, 1995; Weiss et al., 2016). The presence of self-blame and anger in the context of lung cancer is an important consideration when broaching conversations about smoking behavior and recommending appropriate smoking cessation strategies or programs. For example, results from a randomized, controlled trial (Yalcin, Unal, Pirdal, & Karahan, 2014) found that a smoking cessation program that incorporated anger management and stress control strategies significantly reduced the level of stress and anger reported by the study participants and improved sustained quit rates compared to a control group. If the nurse finds that the underlying reason for continued smoking in the context of a lung cancer diagnosis is to help alleviate stress or deal with negative emotions, such as anger, a program of this nature may be more effective in this circumstance to promote and achieve smoking cessation.![]()
Conclusion
This secondary data analysis of a larger dataset was undertaken to enhance understanding of attributions of responsibility for ongoing management of lung cancer and related emotional responses of anger and pride held by affected individuals and FCs. Affected individual and FC judgments of responsibility and emotional reactions of anger toward the affected individual for management of the disease serve as a signal to nurses to intervene by ameliorating the potentially detrimental effects of attributional reactions on psychological health and supportive care within the caregiving dyad. On the other hand, pride in relation to ongoing management of the disease from the perspective of both the affected individual and the FC is also important for nurses to recognize and harness as a source of positive strength and support during the illness experience. This study also provides insight into the attributional and emotional impact of current smoking behavior on the ongoing management of lung cancer. Additional intervention work is required to help position nurses to best respond to complex psychosocial and emotional needs of affected individuals dealing with a stigmatized diagnosis that has a poor prognosis.
About the Author(s)
Deanne J. O’Rourke, RN, MN, GNC(C), is a clinical nurse specialist at Revera LTC and a doctoral candidate in the College of Nursing at the University of Manitoba in Winnipeg, Canada; Michelle M. Lobchuk, RN, PhD, is an associate professor and Manitoba research chair in caregiver communication in the College of Nursing at the University of Manitoba; and Rashid Ahmed, PhD, is an associate professor and associate dean of research in the College of Nursing and Professional Development at the University of North Dakota in Grand Forks. No financial relationships to disclose. Lobchuk completed the data collection. Lobchuk and Ahmed provided statistical support. All authors contributed to the conceptualization and design, provided the analysis, and contributed to the manuscript preparation. O’Rourke can be reached at orourked@myumanitoba.ca, with copy to ONFEditor@ons.org. (Submitted December 2016. Accepted June 27, 2017.)
References
Akechi, T., Okuyama, T., Akizuki, N., Azuma, H., Sagawa, R., Furukawa, T.A., & Uchitomi, Y. (2006). Course of psychological distress and its predictors in advanced non-small cell lung cancer patients. Psycho-Oncology, 15, 463–473. https://doi.org/10.1002/pon.975
American Cancer Society. (2015). Global cancer facts and figures (3rd ed.). Retrieved from http://www.cancer.org/acs/groups/content/@research/documents/document/a…
American Cancer Society. (2016). Cancer facts and figures 2016. Retrieved from https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and…
Canadian Cancer Society’s Advisory Committee on Cancer Statistics. (2015). Canadian cancer statistics 2015. Retrieved from https://www.cancer.ca/~/media/cancer.ca/CW/cancer%20information/cancer%…
Fabrigar, L.R., Wegener, D.T., MacCallum, R.C., & Strahan, E.J. (1999). Evaluating the use of exploratory factor analysis in psychological research. Psychological Methods, 4, 272–299.
Ferlay, J., Soerjomataram, I., Ervik, M., Dikshit, R., Eser, S., Mathers, C., . . . Bray, F. (2013). GLOBOCAN 2012 v1.0, cancer incidence and mortality worldwide: IARC CancerBase No. 11. Lyons, France: International Agency for Research on Cancer. Retrieved from http://globocan.iarc.fr
Folstein, M.F., Folstein, S.E., & McHugh, P.R. (1975). “Mini-mental state.” A practical method for grading the cognitive state of patients for the clinician. Journal of Psychiatric Research, 12, 189–198.
Kassel, J.D., Stroud, L.R., & Paronis, C.A. (2003). Smoking, stress, and negative affect: Correlation, causation, and context across stages of smoking. Psychological Bulletin, 129, 270–304.
Kendall, M., Carduff, E., Lloyd, A., Kimbell, B., Cavers, D., Buckingham, S., . . . Murray, S.A. (2015). Different experiences and goals in different advanced diseases: Comparing serial interviews with patients with cancer, organ failure, or frailty and their family and professional carers. Journal of Pain and Symptom Management, 50, 216–224. https://doi.org/10.1016/j.jpainsymman.2015.02.017
Lehto, R.H. (2007). Causal attributions in individuals with suspected lung cancer: Relationships to illness coherence and emotional responses. Journal of the American Psychiatric Nurses Association, 13, 109–115. https://doi.org/10.1177/1078390307303112
Lehto, R.H. (2007). Causal attributions in individuals with suspected lung cancer: Relationships to illness coherence and emotional responses. Journal of the American Psychiatric Nurses Association, 13, 109–115. https://doi.org/10.1177/1078390307303112
Lehto, R.H. (2014). Patient views on smoking, lung cancer, and stigma: A focus group perspective. European Journal of Oncology Nursing, 18, 316–322. https://doi.org/10.1016/j.ejon.2014.02.003
Lobchuk, M.M., McClement, S.E., McPherson, C.J., & Cheang, M. (2012). Impact of patient smoking behavior on empathic helping by family caregivers in lung cancer [Online exclusive]. Oncology Nursing Forum, 39, E112–E121. https://doi.org/10.1188/12.ONF.E112-E121
Lobchuk, M.M., Murdoch, T., McClement, S.E., & McPherson, C. (2008). A dyadic affair: Who is to blame for causing and controlling the patient’s lung cancer? Cancer Nursing, 31, 435–443. https://doi.org/10.1097/01.NCC.0000339253.68324.19
Luszczynska, A., Pawlowska, I., Cieslak, R., Knoll, N., & Scholz, U. (2013). Social support and quality of life among lung cancer patients: A systematic review. Psycho-Oncology, 22, 2160–2168. https://doi.org/10.1002/pon.3218
Mosher, C.E, Jaynes, H.A., Hanna, N., & Ostroff, J.S. (2013). Distressed family caregivers of lung cancer patients: An examination of psychosocial and practical challenges. Supportive Care in Cancer, 21, 431–437. https://doi.org/10.1007/s00520-012-1532-6
Rudolph, U., Roesch, S., Gritemeyer, T., & Weiner, B. (2004). A meta-analytic review of help giving and aggression from an attributional perspective: Contributions to a general theory of motivation. Cognition and Emotion, 18, 815–848. https://doi.org/10.1080/02699930341000248
Sarna, L., Cooley, M.E., Brown, J.K., Williams, R.D., Chernecky, C., Padilla, G., & Danao, L.L. (2006). Quality of life and health status of dyads of women with lung cancer and family members. Oncology Nursing Forum, 33, 1109–1116. https://doi.org/10.1188/06.ONF.1109-1116
Weiner, B. (1995). Judgments of responsibility: A foundation for a theory of social conduct. New York, NY: Guilford Press.
Weiss, J., Yang, H., Weiss, S., Rigney, M., Copeland, A., King, J.C., & Deal, A.M. (2016). Stigma, self-blame, and satisfaction with care among patients with lung cancer. Journal of Psychosocial Oncology, 35, 166–179. https://doi.org/10.1080/07347332.2016.1228095
Yalcin, B.M., Unal, M., Pirdal, H., & Karahan, T.F. (2014). Effects of an anger management and stress control program on smoking cessation: A randomized controlled trial. Journal of the American Board of Family Medicine, 27, 645–660. https://doi.org/10.3122/jabfm.2014.05.140083
Zhang, A.Y., & Siminoff, L.A. (2003). Silence and cancer: Why do families and patients fail to communicate? Health Communication, 15, 415–429. https://doi.org/10.1207/S15327027HC1504_03


