Parents’ Verbal and Nonverbal Caring Behaviors and Child Distress During Cancer-Related Port Access Procedures: A Time-Window Sequential Analysis
Purpose/Objectives: To study the relationship between parental verbal and nonverbal caring behaviors and child distress during cancer-related port access placement using correlational and time-window sequential analyses.
Design: Longitudinal, observational design.
Setting: Children’s Hospital of Michigan and St. Jude Children’s Research Hospital.
Sample: 43 child–parent dyads, each with two or three video recordings of the child undergoing cancer-related port placement.
Methods: Two trained raters coded parent interaction behaviors and child distress using the Parent Caring Response Scoring System and Karmanos Child Coping and Distress Scale, respectively. Mixed modeling with generalized estimating equations examined the associations between parent interaction behaviors and parent distress, child distress, and child cooperation reported by multiple raters. Time-window sequential analyses were performed to investigate the temporal relationships in parent–child interactions within a five-second window.
Main Research Variables: Parent caring behaviors, child distress, and child cooperation.
Findings: Parent caring interaction behaviors were significantly correlated with parent distress, child distress, and child cooperation during repeated cancer port accessing. Sequential analyses showed that children were significantly less likely to display behavioral and verbal distress following parent caring behaviors than at any other time. If a child is already distressed, parent verbal and nonverbal caring behaviors can significantly reduce child behavioral and verbal distress.
Conclusions: Parent caring behaviors, particularly the rarely studied nonverbal behaviors (e.g., eye contact, distance close to touch, supporting/allowing), can reduce the child’s distress during cancer port accessing procedures.
Implications for Nursing: Studying parent–child interactions during painful cancer-related procedures can provide evidence to develop nursing interventions to support parents in caring for their child during painful procedures.
Jump to a section
Children with cancer undergo repeated painful procedures such as lumbar punctures, bone marrow aspirations, and accessing of ports for regular monitoring of their disease, treatment effectiveness, and treatment-related toxicities or side effects (Blount, Piira, Cohen, & Cheng, 2006; Hockenberry et al., 2011; Pizzo & Poplack, 2010). Children report experiencing more pain and distress related to these procedures than from the cancer itself (Hedström, Haglund, Skolin, & von Essen, 2003). Among survivors, prior experiences with distressing and painful procedures can lead to avoidance of regular primary care and monitoring for adverse effects of their cancer therapies (Pate, Blount, Cohen, & Smith, 1996). Supportive care strategies, such as pharmacologic and nonpharmacologic approaches and combinations of both, have been used to help children effectively cope with repeated procedures (Flowers & Birnie, 2015; Hockenberry et al., 2011; Uman et al., 2013). In addition, attention has been paid to parent–child interactions during such procedures, with a conclusion that parent interaction behaviors during the child’s procedures can affect the child’s pain and distress levels (Blount et al., 1989; Caes, Goubert, et al., 2014; Caes, Vervoort, et al., 2014; Cline et al., 2006). Specifically, parent coping-promoting behaviors (e.g., humor) and commands to use specific coping strategies can reduce children’s pain and distress (Blount, Bunke, Cohen, & Forbes, 2001; Blount et al., 1989). Conversely, parent distress-promoting behaviors, such as empathy, apologies, and reassurance, can exacerbate children’s pain and distress levels during painful procedures (Blount et al., 1989, 2001; Blount, Sturges, & Powers, 1990; Spagrud et al., 2008).
Although the literature provides evidence regarding how parent interaction behaviors affect children’s pain and distress during painful procedures, the findings are inconsistent, particularly regarding distress-related responses (e.g., empathy, reassurance). The results of studies other than Blount et al.’s (1989, 1990) imply that parent empathy and reassurance behaviors may help children cope with cancer-related procedures and lead to lower pain and distress compared to parent distancing and invalidating behaviors (Cline et al., 2006). Some have suggested that reassurance might consist of subconcepts that account for the mixed child outcomes (McMurtry, Chambers, McGrath, & Asp, 2010; McMurtry, McGrath, Asp, & Chambers, 2007). In addition, Penner et al. (2008) investigated two subdomains of parent empathy (e.g., empathy concern, empathy distress) and found that parent empathy concern (e.g., softhearted, warm) negatively correlated with child’s pain and distress during cancer procedures. In the same study, parent empathy distress (e.g., upset, worried) positively correlated with child’s pain and distress during cancer procedures.
Importantly, parent nonverbal behaviors during their child’s painful procedures are rarely studied. In one of the few published studies on this topic, Peterson et al. (2007) found that parent supportive touch significantly reduced child pain and distress during cancer procedures, suggesting that parent nonverbal behaviors can significantly shape a child’s short- and long-term responses to the cancer experience.
Repeated port accessing is an essential element of the childhood cancer experience and is typically performed by nurses with the child’s parent present. Although the literature provides evidence regarding the importance of parent–child interactions during painful procedures (Blount et al., 1989; Caes, Goubert, et al., 2014; Caes, Vervoort, et al., 2014; Cline et al., 2006), most studies investigating parent–child interaction behaviors were cross-sectional rather than longitudinal. In addition, existing studies relied on correlational analyses rather than newer methods, such as time-window sequential analysis (Chorney, Tan, & Kain, 2013). This type of analysis can provide insight into whether the presence of a particular parent interaction behavior increases or decreases the occurrence of another behavior within a particular length of time. Using a theory-based measure to study parents interactions with their child during repeated port accessing and association between parent interaction behaviors and child outcomes can provide a framework to guide parents in supporting their children during port accessing and perhaps other procedures that are repeated on a regular basis during the course of the child’s illness trajectory.
This study used an observational measure based on Swanson’s theory of caring to (a) investigate relationships between parent verbal and nonverbal caring behaviors and child distress and child cooperation over repeated port accessing, and (b) examine temporal relations between parent verbal and nonverbal caring behaviors and child distress over port accessing using the time-window sequential analyses. Swanson’s theory of caring is a middle-range theory originally developed to understand miscarriage and design theory-based interventions for women who have experienced a miscarriage. This theory has been extended to understand parental perceptions and behaviors in taking care of their child in clinical care situations, such as congenital heart disease (Wei et al., 2016) and brain trauma (Roscigno & Swanson, 2011). Swanson’s theory of caring includes five caring processes: knowing, being with, doing for, enabling, and maintaining belief (Swanson, 1991, 1993, 2013). The theory has also been used in multiple healthcare systems as a practice theory (Tonges & Ray, 2011), indicating its application beyond the perinatal loss context from which it was derived.
Methods
This study, which was part of a larger parent study (R01CA138981; principal investigator: L. Penner), used a longitudinal observational design. Data were collected from 2009–2015 at two large pediatric oncology programs in the United States. The parent study was reviewed and approved by the hospitals’ institutional review boards (IRBs) and the university affiliated with one of the hospitals. Study assessments included person-reported outcomes and video recordings of parent–child interactions related to port accessing for a child diagnosed with cancer. This secondary analysis employed parent study data collected at entry to the study (T1) and immediately before and after as many as three cancer-related procedures (T2, T3, and T4). Procedures at T2, T3, and T4 were separated by at least two weeks but no more than three months.
Settings and Sample
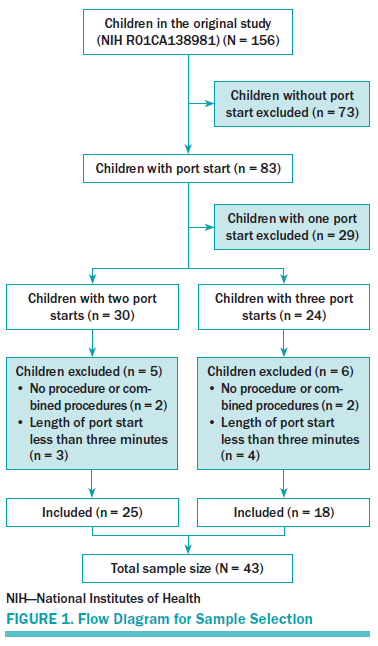
Children and their parents were eligible to enroll in the study if (a) the child’s age was 3–12 years, (b) the child had been diagnosed with cancer at least 1 month but no more than 18 months before study entry and was undergoing regular port accessing, and (c) the parent and child were able to speak English and the parent read English well enough to provide informed consent and complete the questionnaires. One-hundred fifty-six children and their parents enrolled in the parent study. Parents signed informed consent and children aged 4 years and older provided verbal assent. Only those children and their parents who provided data at baseline (T1) and also at least two of the three recorded port accessing procedures (T2, T3, and T4) were included in this analysis. Children and parents were excluded from this study if the child did not undergo port accessing, the port accessing was done in combination with a lumbar puncture or bone marrow aspiration, or the port accessing was accomplished in less than three minutes. Data from 43 children and their parents (one parent per child) were subjected to secondary analysis, including 25 children with two video-recorded port accessing procedures and 18 children with three video-recorded port accessing procedures. Therefore, a total of 104 video-recorded port accessing procedures were subjected to this analysis (see Figure 1). All videos were coded second to second, suggesting an adequate sample size to complete the study aims.
Measures
Parent Caring Response Scoring System: The 18-item Patient Caring Response Scoring System (P-CaReSS) is an observational measure to assess parent caring behaviors toward the child during painful procedures (see Table 1). The development of this measure was informed by Swanson’s theory of caring (Swanson, 1991). The items comprise five caring domains: knowing (one item), being with (three items), doing for (three items), enabling (four items), and maintaining belief (two items) (Swanson, 1991) and one empirically noncaring domain (four items) that capture parent verbal, nonverbal, and emotional behaviors from Swanson’s theory of caring perspective (Bai, 2016). The caring domains are defined by Swanson (1991) as:
• Knowing: Striving to understand an event as it has meaning in the life of the other
• Being with: Being emotionally present to the other
• Doing for: Doing for the other as he/she would do for oneself
• Enabling: Facilitating the other’s passage through life transitions and unfamiliar events
• Maintaining belief: Sustaining faith in the other’s capacity to get through an event or transition and face a future with meaning.
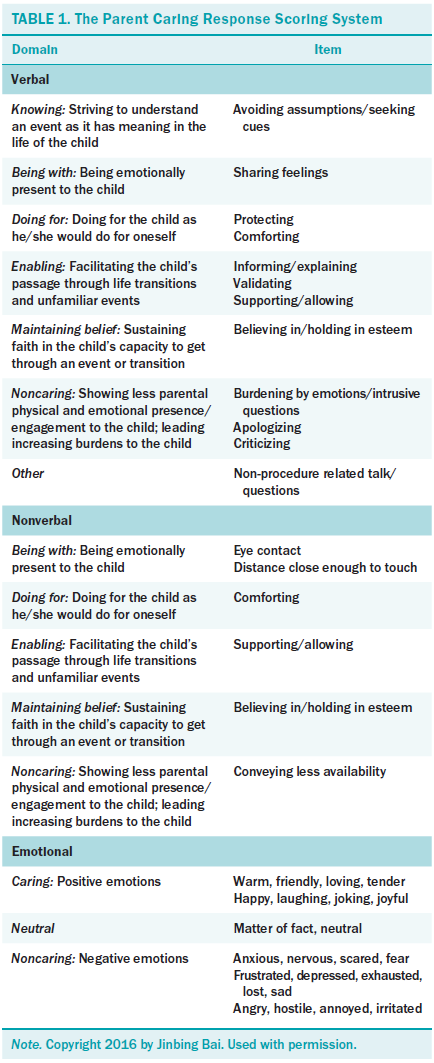
Verbal behaviors are coded as “presence” or “absence,” onset and offset times (i.e., durations) of nonverbal behaviors are coded only if the behaviors occurred, and the emotional behavior score was based on a global impression of a video-recorded session as positive (1), neutral (0), or negative (–1). The P-CaReSS showed good inter-rater reliability with percentage agreements above 80% for the P-CaReSS overall (0.82) and each domain: verbal (0.83), nonverbal (0.8), and emotional (0.91) (Bai, Swanson, Harper, Penner, & Santacroce, 2017).
Karmanos Child Coping and Distress Scale: Harper, Peterson, Taub, Albrecht, and Penner (2014) developed the Karmanos Child Coping and Distress Scale (K-CCD) for use by clinicians to code child coping and distress behaviors during cancer-related procedures. For this study, the two-item distress subscale of the K-CCD was used to code child behavioral and verbal expressions of distress before, during, and following the port accessing. Verbal distress was coded as “presence” or “absence,” and onset and offset times (i.e., durations) of behavioral distress were coded if the behaviors occurred. The distress subscale has acceptable inter-rater reliability with an average percent agreement of 78% between two trained coders.
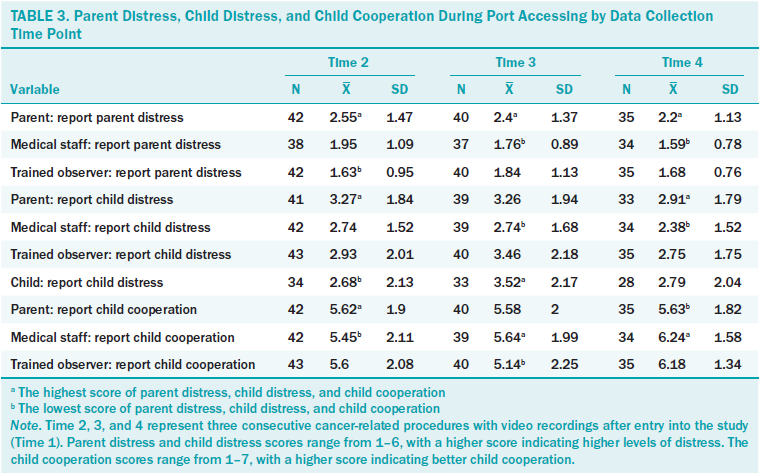
Wong-Baker Faces Scale: The one-item Wong-Baker Faces Scale (W-BFS) was used to evaluate parent distress and child distress during the port accessing. The scale consists of six faces with rating anchors from 1 (no distress at all) to 6 (the worst distress) (Wong & Baker, 1988). After port accessing, parent distress was rated by the parent, clinical staff (e.g., nurses), and a trained research team member. Child distress was rated by the same three raters plus the child. Correlation coefficients ranging from 0.57–0.72 for the W-BFS ratings by parent, clinical staff, child, and trained observer provide support for reliability (Peterson et al., 2014; Trentacosta et al., 2016). Among the multiple raters, parents reported the highest parent distress and child distress scores, and the clinical staff reported the lowest parent distress and child distress scores.
Child Cooperation Scale: The Child Cooperation Scale provides a one-item global rating of child cooperation during procedures. The rating scale is anchored by 1 (totally uncooperative) and 7 (totally cooperative). Correlation coefficients range from 0.51–0.72 for the ratings between parent, clinical staff, and trained observer, and provide support for reliability (Peterson et al., 2014). The clinical staff reported the highest child cooperation score among the multiple raters.
Procedures
Coder training: The first author and one PhD-prepared coder were trained to code the video data under the supervision of two scientists from Wayne State University in Detroit, MI. Both coders received training to use P-CaReSS and K-CCD through StudioCode® software. Eleven videos of port accessing were used to test the inter-rater reliability between both coders. Data coders were sufficiently credentialed to conduct coding when they achieved 80% agreement with the primary coder (Sharpe & Koperwas, 2003). Videos used for the training were excluded from the analysis.
Coding process: Each video of a port accessing was divided into three phases (before, during, and post-procedure) according to Cline et al.’s (2006) work. Video segments (or “thin slices”), such as 30 seconds rather than the whole video, can be used to study interactions during painful procedures (Chorney et al., 2013; Henry & Eggly, 2013). The thin slice method has been shown to increase data coding efficiency with reliability in interaction studies (Ambady, Bernieri, & Richeson, 2000; Henry & Eggly, 2013). In the current study, three distinct three- to five-minute slices, one for each phase described here, were coded for each video: (a) the first five minutes immediately before the initiation of port accessing, (b) a three- to five-minute slice during port accessing, and (c) an additional five minutes or shorter slice after completing the port accessing. The first author prepared the slices for each video before data coding. All 104 videos were randomly assigned to two coders. Each coder viewed the video in full once and then coded parent interaction behaviors (P-CaReSS) and child distress (K-CCD) in multiple passes. Both coders recorded the onset times for parent verbal behaviors in the P-CaReSS and child verbal distress in the K-CCD; the onset and offset times were recorded for parent nonverbal and emotional behaviors in the P-CaReSS, and child behavioral distress in the K-CCD. Both coded the videos independently. Any questions and discrepancies regarding the coding process were resolved by a weekly discussion.
Statistical Analyses
Descriptive statistics were used to summarize sample demographic characteristics and study variables. Means were estimated for the data with approximately normal distributions; otherwise, medians (interquartile range) were used. Number (%) described the categorical data. Because of the non-normal distribution of primary variables, mixed modeling with generalized estimating equations (GEE) was used to estimate associations between parent interaction behaviors and parent distress, child distress, and child cooperation. First, parent distress ratings (by parent, clinical staff, and observer), child distress ratings (by parent, clinical staff, observer, and child), and child cooperation ratings (by parent, clinical staff, and observer) were recoded as 0 or 1 based on the value closest to median percentage (i.e., values within less than 50% were coded as “0” and others were coded as “1”). Based on each estimate and its 95% confidence intervals (CIs) in the mixed modeling, an odds ratio (OR) with 95% CIs was calculated for each correlational analysis.
Time-window sequential analysis was used to examine whether the presence of a particular parent interaction behavior increased or decreased the probability of the occurrence of a child distress behavior within a particular temporal window, which was set between three and five seconds in previous studies (Chorney et al., 2013; Chorney, Garcia, Berlin, Bakeman, & Kain, 2010). Time-window sequential analysis was performed and a conservative time window of within five seconds was used in this study. First, time-window sequential analysis was conducted at the individual dyad level and Yule’s Q score was computed to present how parent interaction behaviors precede or follow child verbal and behavioral distress within a five-second time window. Yule’s Q score ranges from –1 to 1, like the Pearson product-moment correlation, with the strength of negative correlations increasing as the score approaches –1 and the strength of positive correlations increasing as the score approaches 1 (Chorney et al., 2010, 2013). In addition, mean Yule’s Q values were estimated for the whole sample and a binomial test was conducted to examine whether the distribution of Yule’s Q score values differed significantly from the distribution to be expected based on chance. Two sets of sequential analysis were performed by the General Sequential Querier Program (Bakeman & Quera, 1995). The first set of sequential analyses examined whether children were less likely to display behavioral and verbal distress within five seconds after parent interaction behaviors than at any other time; and the second examined parent interaction behaviors during children’s behavioral and verbal distress. Participants must have displayed the parent or child behavior of interest to receive a Yule’s Q score; therefore, sample sizes are different for each analysis.
Results
Descriptive Analyses
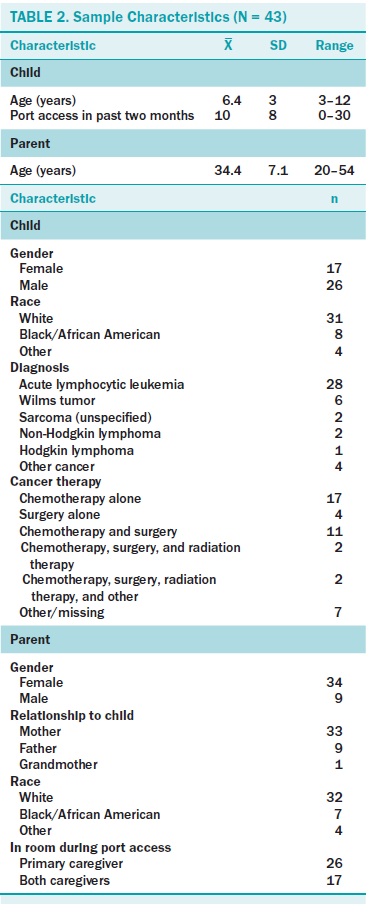
Table 2 shows participants’ demographic and cancer treatment information. Almost all the children (greater than 93%) had received a mixture of local anesthetics (i.e., prilocaine and lidocaine [EMLA]) being applied to the skin over their port area at least 30 minutes before the procedure. Mean durations of the port accessing were 6.08 minutes (SD = 2.21), 6.54 minutes (SD = 2.74), and 6.55 minutes (SD = 2.88) at T2, T3, and T4, respectively. Mean time from the diagnosis to T2 was 6.14 months; mean times between T2 and T3 and between T3 and T4 were 5.27 and 4.31 weeks, respectively.
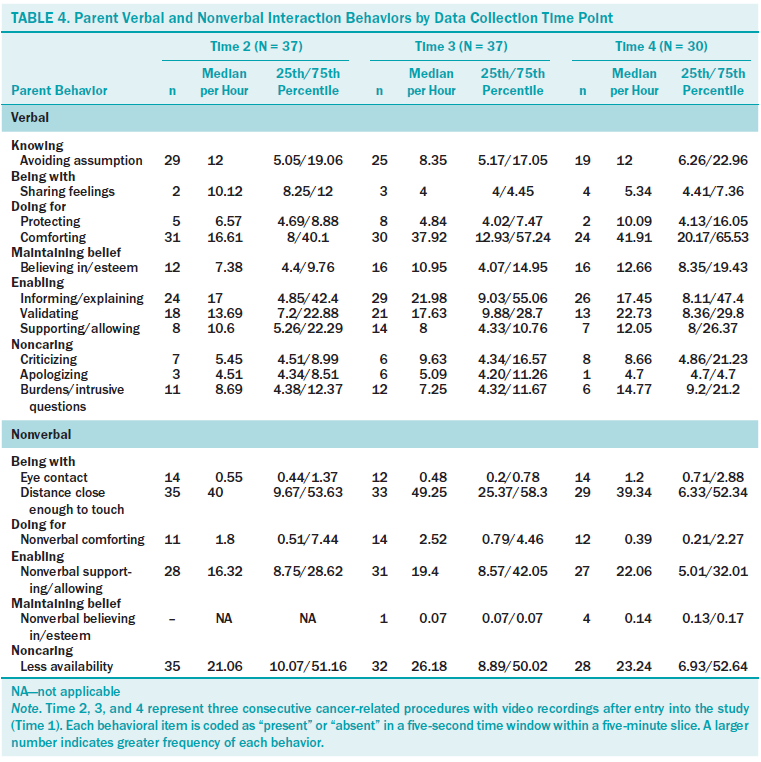
Immediately after each port accessing, parent, clinical staff, and the trained observer reported parent distress, child distress, and child cooperation throughout the whole procedure. Children also reported their distress level. Table 3 presents mean scores for parent distress, child distress, and child cooperation by multiple raters at T2, T3, and T4. Two coders coded the video-recorded data for parent interactions behaviors and child behavioral and verbal distress. Table 4 describes the percentage, median, and 25th/75th percentile for each parent interaction behavior.
Correlational Analyses
Table 5 shows the correlations between the P-CaReSS domains and the ratings of parent distress, child distress, and child cooperation. Positive relationships were found between the P-CaReSS caring domains of parent verbalizations (e.g., enabling, maintaining belief) and nonverbal behaviors (e.g., being with, enabling) and parent distress ratings by multiple raters. Parent verbal expressions of caring (e.g., enabling, knowing) and nonverbal caring behaviors (e.g., being with, enabling) were positively correlated with child distress ratings by multiple raters. Parent nonverbal noncaring behaviors were negatively correlated with parent distress and child distress ratings. Negative relationships were found between caring domains of parent verbal behaviors (e.g., enabling, maintaining belief) and nonverbal behaviors (e.g., being with, enabling) and child cooperation ratings by multiple raters, but positive correlations were found between the parent nonverbal noncaring domain and child cooperation ratings.
Time-Window Sequential Analyses
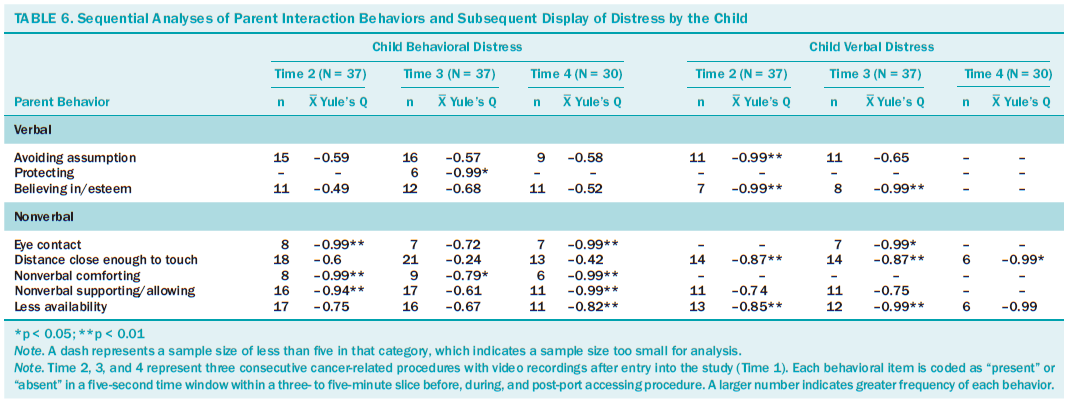
Table 6 shows the temporal relationships between parent interaction behaviors and subsequent child displays of behavioral and verbal distress. A significant proportion of children displayed less behavioral distress following parent nonverbal interaction behaviors—eye contact (mean Yule’s Qs –0.99), comforting (mean Yule’s Qs –0.79 to –0.99), supporting/allowing (mean Yule’s Qs –0.94 to –0.99), and less availability (mean Yule’s Q –0.82)—than at any other time across study time points; children were also less likely to display behavioral distress following parent verbal protecting behavior than at any other time (mean Yule’s Q –0.99). Similarly, a significant proportion of children displayed less verbal distress following parent nonverbal interaction behaviors—eye contact (mean Yule’s Q –0.99), distance close enough to touch (mean Yule’s Qs –0.87 to –0.99), supporting (mean Yule’s Qs –0.94 to –0.99), and less availability (mean Yule’s Qs –0.85 to –0.99)—than at any other time. Children displayed less verbal distress following parent avoiding assumption and believing in/esteem behaviors (mean Yule’s Q –0.99). However, children’s verbal and behavioral distress showed no significant changes following parent verbal noncaring behaviors, such as criticizing and apologizing.
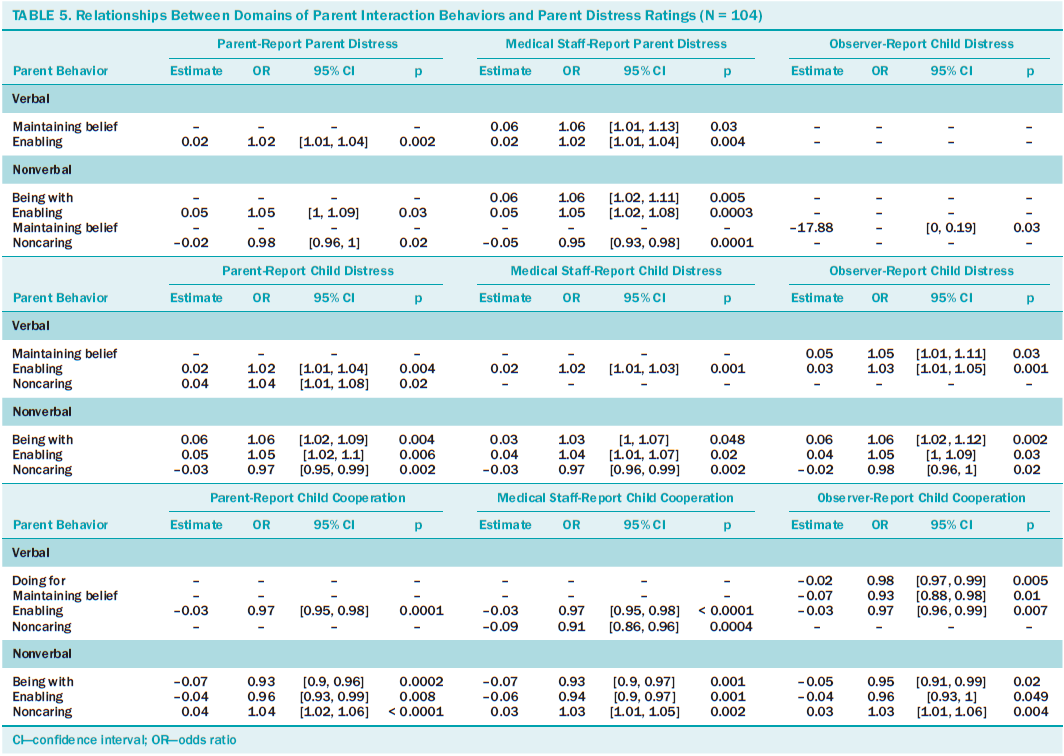
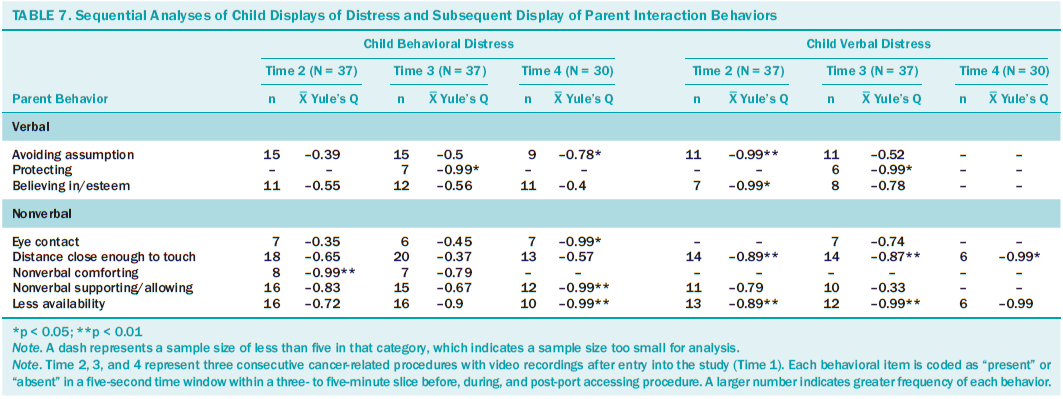
Table 7 shows the temporal relationships between parent interaction behaviors subsequent to child behavioral and verbal displays of distress. Following child behavioral distress, parents displayed fewer nonverbal behaviors—eye contact (mean Yule’s Q –0.99), comforting (mean Yule’s Q –0.99), supporting/allowing (mean Yule’s Q –0.99), and less availability (mean Yule’s Qs –0.9 to –0.99)—than at any other time across time points; parents also displayed fewer avoiding assumption (mean Yule’s Q –0.78) and protecting behaviors (mean Yule’s Q –0.99) while their children were displaying behavioral distress. Similarly, parents displayed fewer nonverbal behaviors following child verbal distress—distance close enough to touch (mean Yule’s Qs –0.87 to –0.99) and less availability (mean Yule’s Qs –0.89 to –0.99)—than at any other time across study time points; when the child displayed verbal distress, the subsequent use of avoiding assumption (mean Yule’s Q –0.99), protecting (mean Yule’s Q –0.99), and believing in/esteem behaviors (mean Yule’s Q –0.99) were less likely to occur than at any other time. No significant temporal correlations were found with respect to parent verbal noncaring behaviors while a child was engaged in behavioral and verbal distress.
Discussion
This study examined relationships between parent verbal and nonverbal behaviors and child distress during repeated port accessing. The authors found that parent verbal and nonverbal caring behaviors but less nonverbal noncaring behaviors were associated with higher parent distress as rated by the parent or higher child distress as rated by the child. Sequential analyses confirmed that parent nonverbal caring behaviors cued lower probability of child verbal and behavioral distress, suggesting that these parent caring behaviors can protect children distress during painful procedures. In addition, parent caring behaviors protected children from distress even when the child was distressed. Studies have reported correlations between parent interaction behaviors and child distress (Chorney et al., 2013; Taylor, Sellick, & Greenwood, 2011), but the temporal relations between parent–child interactions are rarely investigated during repeated cancer procedures.
Parent caring and noncaring behaviors (except less availability) positively correlated with parent distress and child distress but negatively correlated with child cooperation during the port accessing. Less parent availability was negatively correlated with parent distress and child distress but positively correlated with child cooperation. This was the first study to investigate parent interaction behaviors using the Swanson’s theory of caring–based observational measure, and the current results differ from those of previous studies. Previous studies have divided parent interaction behaviors into different types, such as coping-promoting and distress-promoting behaviors, suggesting that distress-promoting behaviors increase child pain and distress, whereas parent coping-promoting behaviors reduce child pain and distress during procedures (Chorney et al., 2013; Taylor et al., 2011). These differences can be interpreted as follows: First, previous studies aimed at distinguishing parent interaction behaviors that contribute to a child’s negative procedure-related responses, such as pain and distress (Blount et al., 2001; Chorney et al., 2013; Taylor et al., 2011). However, the current study attempted to articulate parent interaction behaviors from a theory-based perspective. All parent behaviors were grouped into caring and noncaring domains based on operational definitions and codes. Second, child distress can trigger parent caring and empathic concerns (Noddings, 1984; Penner et al., 2008). In other words, the greater the distress displayed by the child, the greater the caring interaction behaviors evidenced by the parent. Similarly, the greater the cooperation by the child, the fewer the caring interaction behaviors from the parent. Third, parents with greater levels of distress might have more concerns about the procedure as well as its outcomes or results based on their previous experience and the child’s illness situation, which could lead to greater parent interaction behaviors toward their child.
The results of this study suggest that, based on Swanson’s theory of caring, parent interaction behaviors protect the children from distress, particularly parent nonverbal caring behaviors, such as eye contact and being within a distance close enough to touch the child or the child to touch the parent. Conversely, if a child was distressed, the child was less likely to remain distressed when parents used verbal caring behaviors (e.g., avoiding assumption, believing in/esteem) and nonverbal caring behaviors.
This study is the first to explore parent caring behaviors using observational methods to understand the impact of parent caring in domains derived from Swanson’s theory of caring on a child’s distress during repeated cancer-related procedures. The current findings are congruent with previous studies to support the contributions of Swanson’s theory of caring. Swanson et al. (2009) investigated caring-based interventions among women after miscarriage and found that these interventions can reduce women’s overall emotional disturbance, anger, and depression. This study expands the use of Swanson’s theory for studying parent–child interactions during repeated port accessing and provides a foundation to design theory-based interventions to reduce a child’s distress during painful procedures.
Limitations
This study has several limitations. First, the transformation of non-normally distributed continuous variables (e.g., child distress) into categorical variables and use of mixed modeling with GEE simplified the correlations between parent–child interaction behaviors. Second, temporal relationships between parent interaction behaviors and child distress do not imply causation and, therefore, causation cannot be inferred from the findings. Future experimental studies can be developed to examine causality by manipulating significant parent verbal and/or nonverbal caring behaviors. In addition, this study did not examine whether demographic variables (e.g., child age and parent gender) and parent psychological attributes (e.g., parent positive and negative affections) moderate or mediate relationships between parent interaction behaviors and child distress. Future studies should explore moderators of parent interactions behaviors and mediator of child outcomes during repeated painful procedures. Finally, the study did not specifically capture what parents have learned about how to support their child during port accessing and child’s physiologic status (e.g., use of corticosteroid, fever), which should be considered in future studies.
Implications for Nursing
Parent–child interaction is a complex phenomenon that cannot be described in a single dimension. Blount et al. (2008) suggested the necessity to explore this phenomenon via a variety of dimensions, such as verbal, nonverbal, and emotional domains. The current study provides evidence to revisit previous mixed findings regarding the influence of parent behaviors on child treatment responses (i.e., pain, distress, and cooperation) during port accessing using a newer research method (i.e., time-window sequential analysis). All the findings can help nurses and parents identify how parental interaction behaviors affect their child during painful cancer procedures. In addition, findings from this study can advance parent roles in cancer treatment-related procedures and be used to assist healthcare providers and nurse educators in changing clinical practice policy related to nurse-operated procedures, such as port accessing. An adequate addressing of parent behaviors can potentially increase a child’s cooperation and, thereafter, increase nurse work efficiency and efficacy during the procedures. Finally, the current findings have provided a basis for developing nursing interventions that aim to support parents in caring for their child during port accessing and to decrease the negative effects of invasive procedures on child and parent psychological health in the short and long term.
Conclusion
The current study found that processes of Swanson’s theory of caring-derived domains of parent interaction behaviors were significantly associated with parent distress, child distress, and child cooperation, as expected during cancer port accessing. Sequential analyses suggested that parent caring behaviors, particularly rarely studied parent nonverbal behaviors, reduce the child’s behavioral and verbal distress. Similarly, parent caring behaviors can lessen child distress even when the child is distressed. Future theory-based interventions should be designed to facilitate parent use of verbal and nonverbal caring behaviors to minimize child distress during cancer procedures.
The authors gratefully acknowledge Diane Hudson-Barr, PhD, RN, for her review of the manuscript and Vicenç Quera, PhD, for providing statistical assistance.
About the Author(s)
Bai is a postdoctoral fellow in the Nell Hodgson Woodruff School of Nursing at Emory University in Atlanta, GA; Harper is an associate professor and Penner is a professor of oncology, both in the School of Medicine at Wayne State University in Detroit, MI; Swanson is a professor and dean of the College of Nursing at Seattle University in Washington; and Santacroce is an associate professor and the Beerstecher Blackwell Distinguished Scholar in the School of Nursing at the University of North Carolina in Chapel Hill. This research was funded by a research grant awarded to Bai by the Sigma Theta Tau Alpha Alpha Chapter of the University of North Carolina at Chapel Hill School of Nursing, and a research grant (NCIR01CA138981) awarded to Penner from the National Institutes of Health. Harper and Penner completed the data collection. Bai and Harper provided statistical support. Bai and Swanson provided the analysis. All authors contributed to the conceptualization, design, and manuscript preparation. Bai can be reached at jinbing.bai@emory.edu, with copy to editor at ONFEditor@ons.org. Submitted February 2017. Accepted for publication April 11, 2017.
References
Ambady, N., Bernieri, F.J., & Richeson, J.A. (2000). Toward a histology of social behavior: Judgmental accuracy from thin slices of the behavioral stream. In M.P. Zanna (Ed.), Advances in Experimental Social Psychology (pp. 201–272). San Diego, CA: Academic Press.
Bai, J. (2016). Parent distress, parent-child interactions, child distress and child cooperation during cancer treatment-related port starts: A caring perspective [Doctoral dissertation]. University of North Carolina, Chapel Hill. Retrieved from http://search.proquest.com/docview/1806124684
Bai, J., Swanson, K., Harper, F.W.K., Penner, L.A., & Santacroce, S.J. (2017). Parent Caring Response Scoring System: Development and psychometric evaluation in the context of childhood cancer-related port starts. Scandinavian Journal of Caring Sciences. Retrieved from http://onlinelibrary.wiley.com/wol1/doi/10.1111/scs.12504/full
Bakeman, R., & Quera, V. (1995). Analyzing interaction: Sequential analysis with SDIS and GSEQ. Cambridge, UK: Cambridge University Press.
Blount, R.L., Bunke, V., Cohen, L.L., & Forbes, C.J. (2001). The Child-Adult Medical Procedure Interaction Scale–Short Form (CAMPIS-SF): Validation of a rating scale for children’s and adults’ behaviors during painful medical procedures. Journal of Pain and Symptom Management, 22, 591–599.
Blount, R.L., Corbin, S.M., Sturges, J.W., Wolfe, V.V., Prater, J.M., & James, L.D. (1989). The relationship between adults’ behavior and child coping and distress during BMA/LP procedures: A sequential analysis. Behavior Therapy, 20, 585–601. https://doi.org/10.1016/S0005-7894(89)80136-4
Blount, R.L., Piira, T., Cohen, L.L., & Cheng, P.S. (2006). Pediatric procedural pain. Behavior Modification, 30, 24–49. https://doi.org/10.1177/0145445505282438
Blount, R.L., Simons, L.E., Devine, K.A., Jaaniste, T., Cohen, L.L., Chambers, C.T., & Hayutin, L.G. (2008). Evidence-based assessment of coping and stress in pediatric psychology. Journal of Pediatric Psychology, 33, 1021–1045. https://doi.org/10.1093/jpepsy/jsm071
Blount, R.L., Sturges, J.W., & Powers, S.W. (1990). Analysis of child and adult behavioral variations by phase of medical procedure. Behavior Therapy, 21, 33–48. https://doi.org/10.1016/S0005-7894(05)80187-X
Caes, L., Goubert, L., Devos, P., Verlooy, J., Benoit, Y., & Vervoort, T. (2014). The relationship between parental catastrophizing about child pain and distress in response to medical procedures in the context of childhood cancer treatment: A longitudinal analysis. Journal of Pediatric Psychology, 39, 677–686. https://doi.org/10.1093/jpepsy/jsu034
Caes, L., Vervoort, T., Devos, P., Verlooy, J., Benoit, Y., & Goubert, L. (2014). Parental distress and catastrophic thoughts about child pain: Implications for parental protective behavior in the context of child leukemia-related medical procedures. Clinical Journal of Pain, 30, 787–799. https://doi.org/10.1097/ajp.0000000000000028
Chorney, J.M., Garcia, A.M., Berlin, K.S., Bakeman, R., & Kain, Z.N. (2010). Time-window sequential analysis: An introduction for pediatric psychologists. Journal of Pediatric Psychology, 35, 1061–1070. https://doi.org/10.1093/jpepsy/jsq022
Chorney, J.M., Tan, E.T., & Kain, Z.N. (2013). Adult-child interactions in the postanesthesia care unit: Behavior matters. Anesthesiology, 118, 834–841. https://doi.org/10.1097/ALN.0b013e31827e501b
Cline, R.J., Harper, F.W., Penner, L.A., Peterson, A.M., Taub, J.W., & Albrecht, T.L. (2006). Parent communication and child pain and distress during painful pediatric cancer treatments. Social Science and Medicine, 63, 883–898. https://doi.org/10.1016/j.socscimed.2006.03.007
Flowers, S.R., & Birnie, K.A. (2015). Procedural preparation and support as a standard of care in pediatric oncology. Pediatric Blood and Cancer, 62(Suppl. 5), S694–S723. https://doi.org/10.1002/pbc.25813
Harper, F.W.K., Peterson, A.M., Taub, J.W., Albrecht, T.L., & Penner, L. (2014). Observational study of children’s coping and distress during oncology treatment. Annals of Behavioral Medicine, 42.
Hedström, M., Haglund, K., Skolin, I., & von Essen, L. (2003). Distressing events for children and adolescents with cancer: Child, parent, and nurse perceptions. Journal of Pediatric Oncology Nursing, 20, 120–132. https://doi.org/10.1053/jpon.2003.76
Henry, S.G., & Eggly, S. (2013). The effect of discussing pain on patient-physician communication in a low-income, black, primary care patient population. Journal of Pain, 14, 759–766. https://doi.org/10.1016/j.jpain.2013.02.004
Hockenberry, M.J., McCarthy, K., Taylor, O., Scarberry, M., Franklin, Q., Louis, C.U., & Torres, L. (2011). Managing painful procedures in children with cancer. Journal of Pediatric Hematology/Oncology, 33, 119–127. https://doi.org/10.1097/MPH.0b013e3181f46a65
McMurtry, C.M., Chambers, C.T., McGrath, P.J., & Asp, E. (2010). When “don’t worry” communicates fear: Children’s perceptions of parental reassurance and distraction during a painful medical procedure. Pain, 150, 52–58. https://doi.org/10.1016/j.pain.2010.02.021
McMurtry, C.M., McGrath, P.J., Asp, E., & Chambers, C.T. (2007). Parental reassurance and pediatric procedural pain: A linguistic description. Journal of Pain, 8, 95–101. https://doi.org/10.1016/j.jpain.2006.05.015
Noddings, N. (1984). Caring: A feminine approach to ethics and moral education. Berkeley, CA: University of California Press.
Pate, J.T., Blount, R.L., Cohen, L.L., & Smith, A.J. (1996). Childhood medical experience and temperament as predictors of adult functioning in medical situations. Children’s Health Care, 25(4), 281–296. http://doi.org/10.1207/s15326888chc2504_4
Penner, L.A., Cline, R.J., Albrecht, T.L., Harper, F.W., Peterson, A.M., Taub, J.M., & Ruckdeschel, J.C. (2008). Parents’ empathic responses and pain and distress in pediatric patients. Basic and Applied Social Psychology, 30, 102–113. https://doi.org/10.1080/01973530802208824
Peterson, A.M., Cline, R.J., Foster, T.S., Penner, L.A., Parrott, R.L., Keller, C.M., . . . Albrecht, T.L. (2007). Parents’ interpersonal distance and touch behavior and child pain and distress during painful pediatric oncology procedures. Journal of Nonverbal Behavior, 31(2), 79–97. https://doi.org/10.1007/s10919-007-0023-9
Peterson, A.M., Harper, F.W., Albrecht, T.L., Taub, J.W., Orom, H., Phipps, S., & Penner, L.A. (2014). Parent caregiver self-efficacy and child reactions to pediatric cancer treatment procedures. Journal of Pediatric Oncology Nursing, 31, 18–27. https://doi.org/10.1177/1043454213514792
Pizzo, P.A., & Poplack, D.G. (2010). Principles and practice of pediatric oncology (6th ed.). Philadelphia, PA: Lippincott Williams and Wilkins.
Roscigno, C.I., & Swanson, K.M. (2011). Parents’ experiences following children’s moderate to severe traumatic brain injury: A clash of cultures. Qualitative Health Research, 21, 1413–1426.
Sharpe, T., & Koperwas, T. (2003). Behavior and sequential analyses: Principles and practice. Thousand Oaks, CA: Sage.
Spagrud, L.J., von Baeyer, C.L., Ali, K., Mpofu, C., Fennell, L.P., Friesen, K., & Mitchell, J. (2008). Pain, distress, and adult-child interaction during venipuncture in pediatric oncology: An examination of three types of venous access. Journal of Pain and Symptom Management, 36, 173–184. https://doi.org/10.1016/j.jpainsymman.2007.10.009
Swanson, K.M. (1991). Empirical development of a middle range theory of caring. Nursing Research, 40(3), 161–166.
Swanson, K.M. (1993). Nursing as informed caring for the well-being of others. Image: The Journal of Nursing Scholarship, 25, 352–357.
Swanson, K.M. (1999). Effects of caring, measurement, and time on miscarriage impact and women’s well-being. Nursing Research, 48, 288–298.
Swanson, K.M. (2013). A program of research on caring. In M.E. Parker (Ed.), Nursing theories and nursing practice (2nd ed., pp. 351–359). Philadelphia, PA: F.A. Davis Co.
Swanson, K.M., Chen, H.T., Graham, J.C., Wojnar, D.M., & Petras, A. (2009). Resolution of depression and grief during the first year after miscarriage: A randomized controlled clinical trial of couples-focused interventions. Journal of Women’s Health, 18, 1245–1257. doi:10.1089/jwh.2008.1202
Taylor, C., Sellick, K., & Greenwood, K. (2011). The influence of adult behaviors on child coping during venipuncture: A sequential analysis. Research in Nursing and Health, 34, 116–131.
Tonges, M., & Ray, J. (2011). Translating caring theory into practice: The Carolina Care Model. Journal of Nursing Administration, 41, 374–381. https://doi.org/10.1097/NNA.0b013e31822a732c
Trentacosta, C.J., Harper, F.W., Albrecht, T.L., Taub, J.W., Phipps, S., & Penner, L.A. (2016). Pediatric cancer patients’ treatment-related distress and longer-term anxiety: An individual differences perspective. Journal of Developmental and Behavioral Pediatrics, 37, 753–761. https://doi.org/10.1097/dbp.0000000000000327
Uman, L.S., Birnie, K.A., Noel, M., Parker, J.A., Chambers, C.T., McGrath, P.J., & Kisely, S.R. (2013). Psychological interventions for needle-related procedural pain and distress in children and adolescents. Cochrane Database of Systematic Reviews, 10, CD005179. https://doi.org/10.1002/14651858.CD005179.pub3
Wei, H., Roscigno, C.I., Swanson, K.M., Black, B.P., Hudson-Barr, D., & Hanson, C.C. (2016). Parents’ experiences of having a child undergoing congenital heart surgery: An emotional rollercoaster from shocking to blessing. Heart and Lung, 45, 154–160. https://doi.org/10.1016/j.hrtlng.2015.12.007
Wong, D.L., & Baker, C.M. (1988). Pain in children: Comparison of assessment scales. Pediatric Nursing, 14, 9–17.