Integrative Literature Review on Psychological Distress and Coping Strategies Among Survivors of Adolescent Cancer
Problem Identification: Cancer survivors, particularly those diagnosed in adolescence, are faced with physical, mental, and emotional stressors associated with the disease and its treatment. These stressors add to the demand placed on survivors’ already taxed coping skills. This article reviews the literature on psychological distress experienced by survivors diagnosed with cancer during adolescence and the coping strategies they employed.
Literature Search: Three electronic databases (CINAHL®, PsycINFO®, PubMed®) were searched, and 19 studies were selected. Garrard’s matrix method guided this integrative review.
Data Evaluation: Gough’s weight of evidence framework was used to evaluate each study.
Synthesis: Analysis revealed important findings about the types of coping strategies used by adolescents during and after cancer treatment and the impact of each on levels of psychological distress.
Implications for Practice: Healthcare providers, who regularly assess for negative thoughts and unmet needs among survivors, may identify symptoms of psychological distress, intervene early, and facilitate better outcomes for their patients. Patient-centered interventions aimed at coping with psychological distress are most helpful.
Jump to a section
Advances in cancer treatment have increased the overall five-year survival rate to almost 85% (Howlader et al., 2020). However, cancer remains the second leading cause of death for children and adolescents (Howlader et al., 2020). About 5,000–6,000 adolescents aged 15–19 years are diagnosed with cancer annually, and about 500–600 adolescents die from cancer each year (American Cancer Society, 2020). Adolescents are aware of these mortality statistics, and they experience fear and anxiety about their chance of surviving the disease, according to national survey data (Hølge-Hazelton et al., 2016). Because adolescence is a time of dramatic growth in various domains, including physical, cognitive, psychological, and social (Smith et al., 2013), adolescents with cancer face unique challenges in coping with life-threatening illness. Navigating the typical changes of adolescence is difficult; adding cancer-related psychological distress, powerlessness, and insecurity about the future places a heavy demand on teenagers’ coping skills (Ander et al., 2018). To effectively manage stressors, patients with cancer need to learn and employ personal coping strategies, including leaning on others for social support.
Coping is defined as a dynamic process of making cognitive and behavioral choices to reduce stress during cancer treatment; this definition is based on a framework by Folkman and Lazarus (1988). Coping mediates the impact of stressors on physical health and encourages the psychological adjustment that takes place after a cancer diagnosis (Lazarus & Folkman, 1984). During the coping process, primary and secondary appraisals occur. Primary appraisals involve developing strategies to directly change the source of the stress using problem-focused or emotion-focused coping. Problem-focused coping actively aims to change the environment by seeking information and solving problems. Emotion-focused coping aims to change the way one thinks or feels about a stressful situation and involves venting feelings, experiencing denial, and seeking social support. Secondary appraisals focus on the cognitive process of appraising the situation and controlling the situation to the extent possible using secondary control coping strategies (Lazarus & Folkman, 1984). Secondary control coping strategies include relaxing, seeking social support and distraction, and restructuring cognition to manage distress (Hildenbrand et al., 2014). Other secondary ways of coping include avoidant coping strategies in which individuals simply try to stop thinking about a stressful situation to stop experiencing it (Carver et al., 1989); such individuals withdraw and suppress emotional responses (Roth & Cohen, 1986).
Many studies have focused on the psychological distress experienced by and coping strategies of children with cancer (Compas et al., 2015; Monti et al., 2017), young adults with cancer (Michel et al., 2010; Trevino et al., 2012; Xie et al., 2017), and their families. Findings indicate that parents who have a child with cancer use primary coping strategies (e.g., problem-solving, emotion modulation) and secondary control coping strategies (e.g., acceptance). These strategies are associated with lower depressive symptoms (Compas et al., 2015).
In addition, parents’ use of secondary control coping strategies was found to be correlated with their children’s secondary control coping strategies. Parents’ coping strategies after their children’s cancer diagnoses may contribute to how and how well their children cope with cancer-related stress (Monti et al., 2017). In studies of adult-onset cancers, including breast, prostate, and colorectal cancer, survivors used problem- and emotion-focused coping strategies, such as accepting their diagnoses and engaging in physical activities that provided social and emotional support. These coping strategies were associated with less psychological distress, better physical health, and better quality of life (Lashbrook et al., 2018; Tojal & Costa, 2015). Adults with cancer who were psychologically distressed were more anxious and prone to feelings of hopelessness (Kang & Son, 2019). Psychological distress refers to emotional suffering, such as depression and anxiety, that can be associated with physiological symptoms (Drapeau et al., 2012).
Previous studies of children and adolescents with cancer have shown that coping strategies, such as relaxation, emotional expression, and support seeking, were associated with better psychological adjustment (Aldridge & Roesch, 2007; Compas et al., 2012). These coping strategies promote adaptation to a “new normal” for individuals diagnosed with chronic illnesses including cancer, and they result in better health outcomes (Aldridge & Roesch, 2007; Compas et al., 2012). Although relaxation, emotional expression, and support seeking promote psychological adjustment to a cancer diagnosis and concordance with treatment protocols, avoidance as a coping mechanism has the opposite effect (van Dijk et al., 2009; Wu et al., 2013). Survivors may move through various strategies over time, but the prolonged use of avoidance increases psychological distress. This, in turn, manifests itself as anxiety, depression, demotivation, irritability, aggression, or self-deprecation (Compas et al., 2012; Massé, 2000).
It is important to note that the experiences and psychological needs of adolescents with cancer differ from those of children or adults diagnosed with cancer (Smith et al., 2013). Few studies have addressed coping strategies with a focus specifically on adolescents with cancer. Adolescence is a critical period of development that involves dramatic physical and psychological changes, and psychological distress is different for adolescent survivors than for their older and younger counterparts (Berk & Meyers, 2015). The good news is that several studies of long-term survivors of childhood cancer suggest that after a period of adjustment, most survivors become as psychologically healthy as typical individuals of a similar age. However, as many as 20% of survivors report significant psychological distress, including symptoms of depression, anxiety, and somatization (Krull et al., 2010; Smith et al., 2013).
Studies show that undetected or untreated psychological distress during adolescence contributes to health issues in later life, such as obesity, poor health practices, secondary cancer, suicide ideation, and early mortality (Krull et al., 2010; Recklitis et al., 2010). A better understanding of adolescents’ psychological distress and coping mechanisms is important to help adolescents survive and thrive after a life-threatening illness and may have application for adolescents over the course of their lives. This integrative review examines factors associated with psychological distress and the most effective coping strategies for cancer survivors diagnosed during adolescence. An individual diagnosed with cancer is designated as a cancer survivor from the time of diagnosis until the end of life (National Cancer Institute, n.d.). The research questions of this review are as follows: (a) What factors are associated with psychological distress and/or coping strategies? and (b) Which types of coping strategies are associated with lower levels of psychological distress among survivors of adolescent cancer?
Methods
Design
This integrative review followed Garrard’s (2016) matrix method in four steps:
• Databases were searched using keywords.
• Articles were chosen after a review of titles and abstracts.
• Articles were read carefully, with a matrix created that included a summary of each article’s findings.
• Studies were analyzed for similarities and differences in methods and findings.
These four steps are similar to those of other review methods, but the matrix method was specifically designed for health science literature reviews (Garrard, 2016). Authors can create a versatile review matrix that consists of author/title/journal, purpose, research design, methodologic design, findings, and limitations that fits a review’s purpose (Garrard, 2016). The matrix method is an objective review process that synthesizes findings from selected references (Klopper et al., 2007). The quality of each article selected was assessed using Gough’s (2007) weight of evidence (WoE) framework.
Search Methods
The framework of the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement was used to guide the review process (Moher et al., 2009). The search for quantitative and qualitative articles was conducted by the first author (H.S.) and a medical librarian using the electronic databases CINAHL®, PsycINFO®, and PubMed®. The search was limited to articles published from 2000 through December 2019 and the following keywords and their combinations: psychological distress, anxiety or distress, cope, coping strategy, adolescent with cancer, and adolescent cancer survivor. Specific journal and ancestry searches were also conducted. A PRISMA diagram illustrates this process (see Figure 1). 
To be included in the review, studies had to be written in English; be published in a peer-reviewed journal; include diagnoses of childhood-specific cancers (e.g., leukemia, brain or spinal cord tumors, neuroblastoma, Wilms tumor, Hodgkin lymphoma, non-Hodgkin lymphoma, osteosarcoma) in individuals aged 10–19 years, per the World Health Organization’s (n.d.) definition of adolescence; have adolescents comprising at least half of the sample; focus on assessment of coping strategies or relationships between coping strategies and psychological distress; and measure coping-related strategies reported by adolescents with cancer. Studies were excluded if they focused on a specific treatment period (e.g., post–stem cell transplantation) or on coping strategies for other age groups or families of adolescents with cancer.
Data Extraction and Analysis
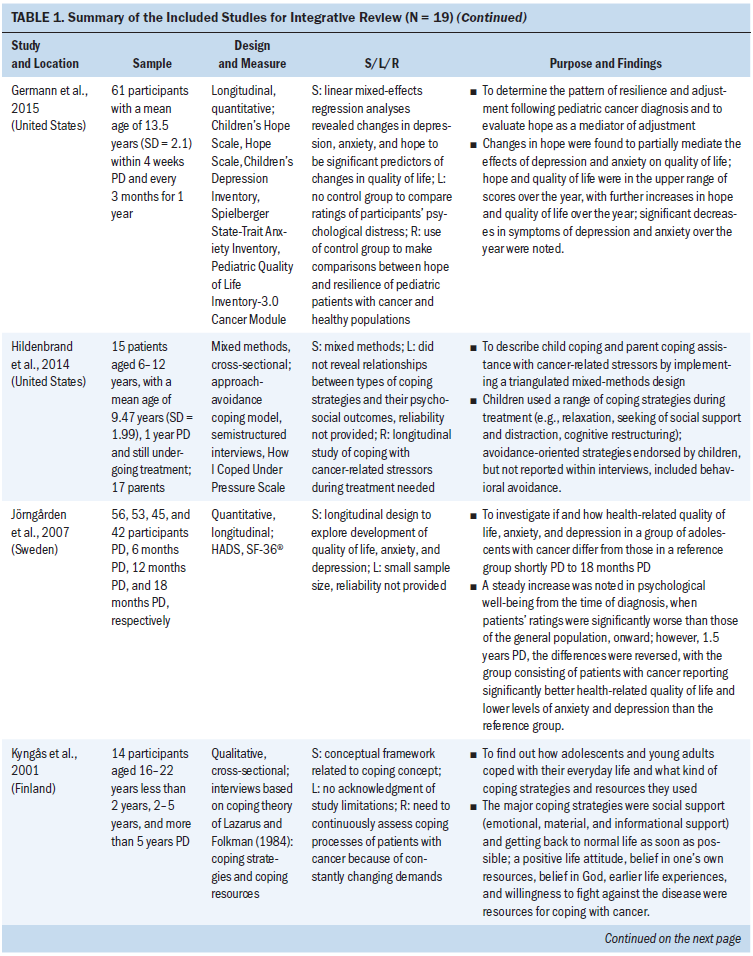
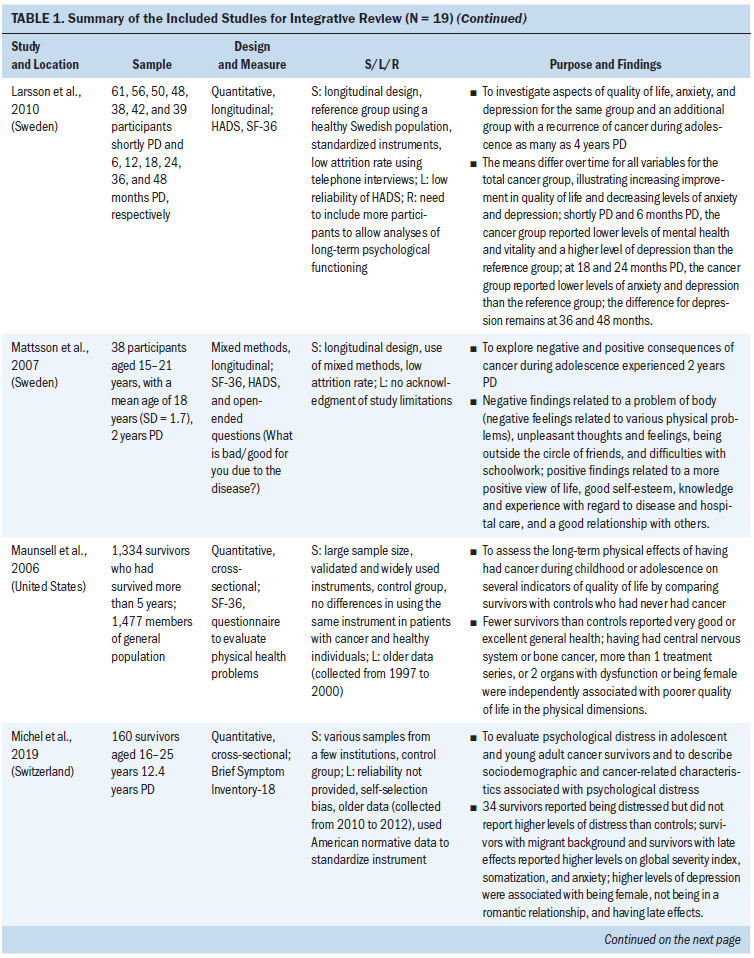
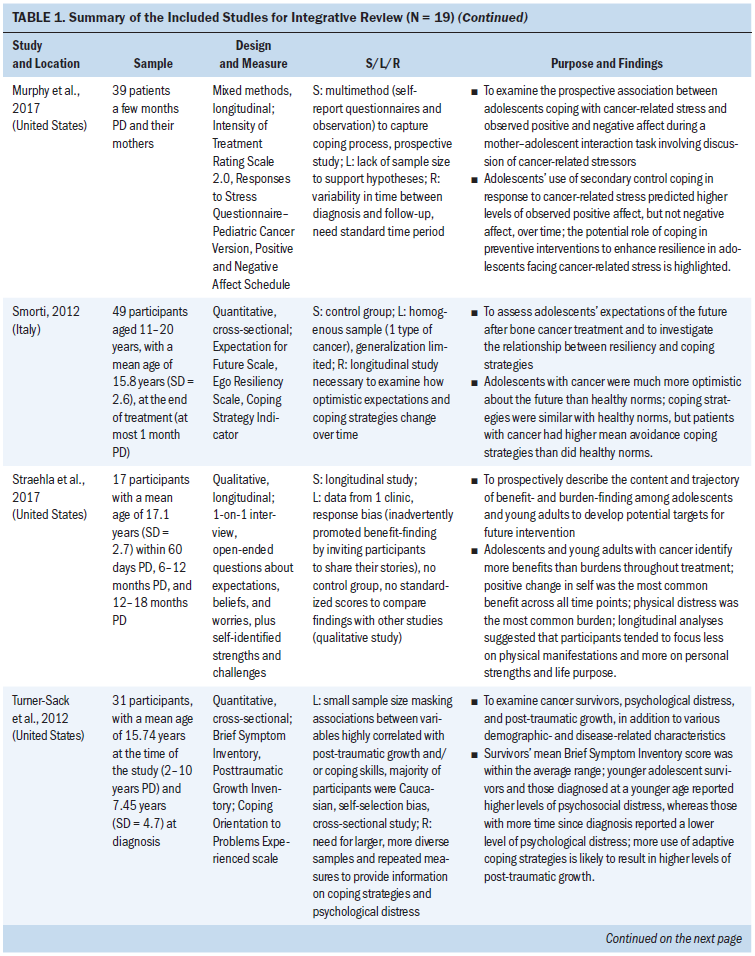
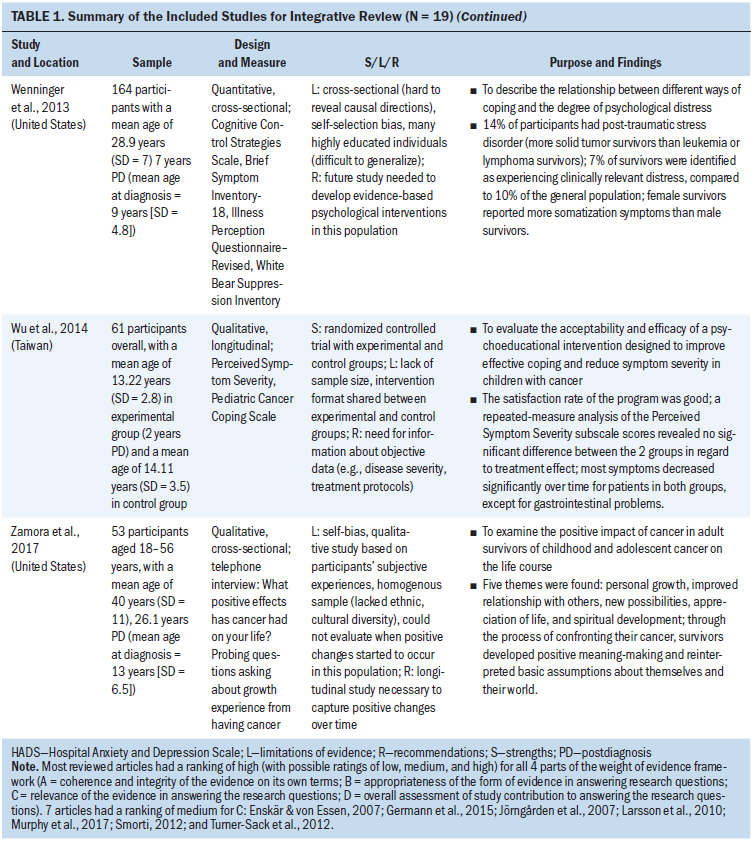
The search resulted in 1,838 journal articles. Of these articles, 279 were duplicates, and 1,403 were excluded because they did not meet inclusion criteria. An additional 137 articles were excluded because the content included only symptoms related to cancer or cancer treatment (n = 46), focused on survivorship care plans (n = 25), focused on research methods (n = 29), focused on health outcomes other than coping (n = 23), or was from the perspective of clinicians or families of children with cancer (n = 14). Ultimately, 19 studies were selected for this review (see Table 1). Information on study purpose, design, sample size, time since diagnosis, measure(s), findings, quality appraisal, and limitations was abstracted and entered into the matrix. 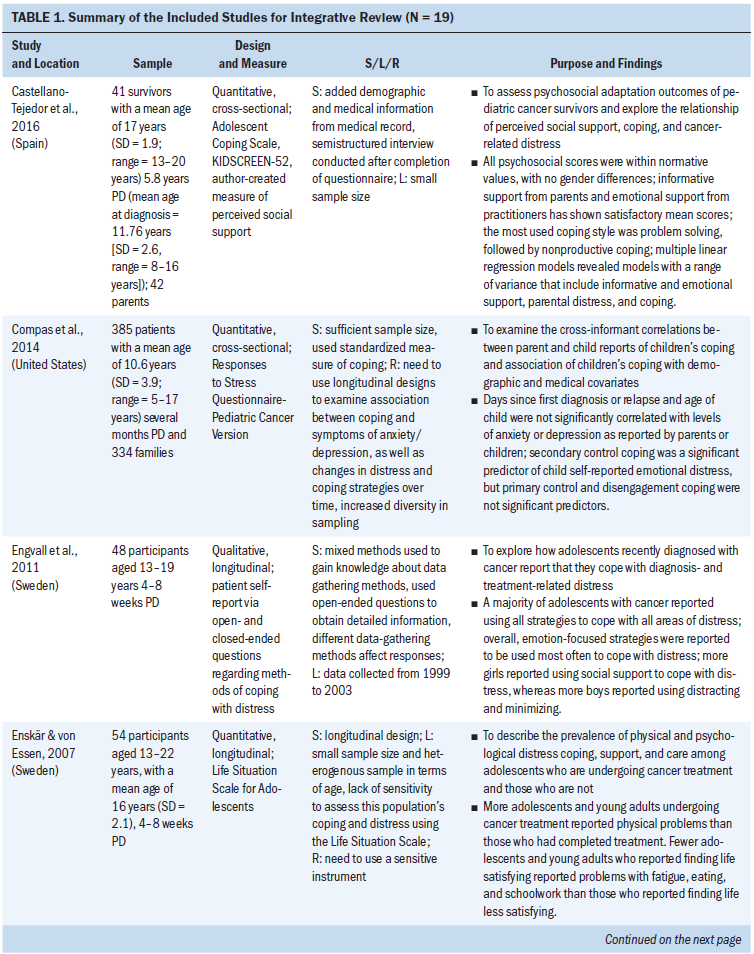
Quality Appraisal
Each article was weighted (high/medium/low) for its overall contribution to answering a research question using the WoE tool (Gough, 2007). Each study’s research design, data collection method, data analysis, claims and evidence, and findings were evaluated using the WoE’s four categories:
• WoE-A is a judgment about the coherence and integrity of the evidence, including clarity of purpose, accuracy, and accessibility of execution of the study.
• WoE-B is a judgment about the appropriateness of the method used, including research design.
• WoE-C is a judgment about the focus of the study and its relevance to review questions, including types of sampling, data analysis, and legal and ethical aspects.
• WoE-D is an overall judgment about how a study answers the review questions.
When a study receives more than two high ratings from WoE-A to WoE-C, then WoE-D is rated as high. Two authors (H.S., J.C.D.) conducted the quality appraisal using the WoE tool. Any disagreement was resolved by consensus or additional discussion.
Results
Among the 19 studies, 11 were quantitative, 5 were qualitative, and 3 used a mixed-methods design. Ten studies used a cross-sectional design, and eight studies were longitudinal. The sample sizes of the studies ranged from 14 to 1,334. Studies were conducted in the United States (n = 9), Sweden (n = 5), Finland (n = 1), Italy (n = 1), Spain (n = 1), Switzerland (n = 1), and Taiwan (n = 1). In most of the studies, the age range of participants was 10–22 years. The studies examined survivors at different stages after cancer diagnosis: immediately following a cancer diagnosis to 1 year after (n = 6) (Compas et al., 2014; Engvall et al., 2011; Enskär & von Essen, 2007; Germann et al., 2015; Hildenbrand et al., 2014; Murphy et al., 2017), 1–5 years after diagnosis (n = 7) (Jörngården et al., 2007; Kyngäs et al., 2001; Larsson et al., 2010; Mattson et al., 2007; Smorti, 2012; Straehla et al., 2017; Wu et al., 2014), 5–10 years after diagnosis (n = 4) (Castellano-Tejedor et al., 2016; Maunsell et al., 2006; Turner-Sack et al., 2012; Wenninger et al., 2013), and more than 10 years after diagnosis (n = 2) (Michel et al., 2019; Zamora et al., 2017).
Some of the studies included descriptive findings of psychological distress and coping strategies. Studies reported the types of coping strategies used (n = 7), psychological and/or physical distress and coping strategies (n = 6), and quality of life and psychological distress (n = 6). Using Gough’s (2007) WoE quality appraisal, two authors (H.S., J.C.D.) agreed initially on 93% of the article classifications and ultimately reached agreement on the remainder. Using the WoE framework, all 19 studies were rated high on the overall assessment (WoE-D) of study quality.
Measurements of Coping Strategies and Psychological Distress
The selected studies used measurement instruments previously validated in studies of adolescents with cancer. Instruments used included the Adolescent Coping Scale (Castellano-Tejedor et al., 2016), the Responses to Stress Questionnaire-Pediatric Cancer Version (Compas et al., 2014; Murphy et al., 2017), the Life Situation Scale for Adolescents (Enskär & von Essen, 2007), the Cognitive Control Strategies Scale (Wenninger et al., 2013), and the Coping Orientation to Problems Experienced scale (Turner-Sack et al., 2012). Five studies used open-ended questions in interviews to ask how participants experienced distress and semistructured interviews to assess coping strategies. The most frequently used psychological distress measurement tool was the Hospital Anxiety and Depression Scale, which was used in three studies (Jörngården et al., 2007; Larsson et al., 2010; Mattsson et al., 2007). The Brief Symptom Inventory was used in three studies (Michel et al., 2019; Turner-Sack et al., 2012; Wenninger et al., 2013). To measure quality of life, four studies used the SF-36® (Jörngården et al., 2007; Larsson et al., 2010; Mattsson et al., 2007; Maunsell et al., 2006).
Four major findings emerged from these studies. Among adolescents, psychological distress is prevalent immediately after cancer diagnosis. Four types of coping strategies were identified: problem-focused coping, emotion-focused coping, avoidant coping, and secondary control coping. Some demographic factors were associated with higher psychological distress, and certain types of coping strategies were associated with lower psychological distress.
Prevalence of Psychological Distress
A cancer diagnosis during adolescence is a significant stressor affecting adolescents’ physical, psychological, and social development (Castellano-Tejedor et al., 2016). Studies found that psychological distress was evidenced by anxiety and depressive symptoms (Compas et al., 2014; Germann et al., 2015; Jörngården et al., 2007; Larsson et al., 2010; Michel et al., 2019; Turner-Sack et al., 2012), unpleasant thoughts and feelings, and difficulties with school work (Enskär & von Essen, 2007; Mattsson et al., 2007). Physical symptoms because of cancer treatment, such as mucositis, pain, eating problems, or fatigue, were also associated with psychological distress (Enskär & von Essen, 2007).
Relationships Between Demographic Characteristics and Psychological Distress
Several factors, such as current age, age at diagnosis, gender, and time since diagnosis, were associated with varying degrees of psychological distress. Adolescents with cancer who were diagnosed at younger ages had higher levels of observed anxiety compared to those diagnosed at older ages (Murphy et al., 2017). The time elapsed since cancer diagnosis and completion of treatment was correlated with lower levels of psychological distress (Jörngården et al., 2007; Larsson et al., 2010; Straehla et al., 2017), so time elapsed since cancer diagnosis is a significant factor associated with decreased psychological distress.
After a period of adjustment, some individuals with cancer had better psychological outcomes than healthy controls or their siblings (Maunsell et al., 2006; Smorti, 2012). In a study by Smorti (2012), bone tumor survivors reported themselves as more optimistic than healthy adolescents, which might be related to these survivors’ resilience. Resilience of adolescents who are diagnosed with cancer is defined as “a process for identifying and developing resources or strengths to manage stresses in order to gain positive outcomes from the experience” (Haase et al., 1999, p. 125). This finding by Smorti (2012) is similar to that noted in a study of children with cancer by Kim and Yoo (2010), which determined that these survivors often manifested notable resilience. Also, use of secondary control coping strategies regarding cancer-related stress was associated with the positive affect of cancer experience (Murphy et al., 2017). Among survivors of adolescent cancer (five or more years since cancer diagnosis), being unemployed and having a romantic relationship were associated with higher levels of depression and anxiety (Michel et al., 2019). Female survivors reported more depressive and somatization symptoms, as well as poorer psychological outcomes, than male survivors (Maunsell et al., 2006; Michel et al., 2019; Turner-Sack et al., 2012; Wenninger et al., 2013). This is similar to the finding that the prevalence of depression and anxiety is two times greater in female adolescents than in male adolescents (Avenevoli et al., 2015; Merikangas et al., 2010).
The type of cancer also plays a role in psychological stress levels. Solid tumor survivors (e.g., bone tumors, soft tissue sarcomas) reported more post-traumatic stress disorder (PTSD) (26%) than hematology tumor survivors (e.g., leukemia, lymphoma) (11%) (Wenninger et al., 2013). Solid tumor treatments may involve surgery or amputation of the affected body area, so changed physical appearance, including loss of a body part or scars, may have a negative effect on self-perceived physical attractiveness among adolescents and young cancer survivors (Olsson et al., 2018). Higher psychological distress scores were also reported by survivors who had at least one medical late effect, such as a complication from cancer treatment (Michel et al., 2019; Wenninger et al., 2013).
Time since diagnosis was a factor in the effects of cancer on adolescents and how they coped. In studies of individuals within two months of cancer diagnosis, most adolescents reported various types of physical and psychological distress, including fatigue, pain, hair loss, nausea, feelings of isolation, worries, physical appearance changes (Engvall et al., 2011; Enskär & von Essen, 2007), and higher levels of depression and anxiety (Compas et al., 2014; Jörngården et al., 2007). Six months after diagnosis, adolescents’ levels of anxiety and depression were higher than those reported by healthy controls (Germann et al., 2015; Jörngården et al., 2007; Larsson et al., 2010). However, survivors reported a decrease in depression and anxiety one year after diagnosis, and these symptoms continued to decrease (Jörngården et al., 2007; Larsson et al., 2010).
Germann et al. (2015) used a longitudinal design to examine psychological distress in the year after cancer diagnosis and found that a similar pattern emerged: Psychological distress decreased from six months to one year following a cancer diagnosis. A few years after cancer diagnosis, psychological distress levels stabilized. Four years after diagnosis, survivors reported lower levels of anxiety and depression and higher levels of vitality than healthy controls (Larsson et al., 2010). Five to seven years after cancer diagnosis, most cancer survivors’ psychological distress scores were similar to those of healthy controls (Castellano-Tejedor et al., 2016; Wenninger et al., 2013). However, a number of survivors still suffered from psychological distress after several years: 17% of cancer survivors reported experiencing clinically relevant distress, compared to 10% of a healthy control group (Wenninger et al., 2013).
Other studies examined the relationship among physical distress, psychological distress, hope, and quality of life based on time since diagnosis. Immediately after a cancer diagnosis to two years after, 44% of cancer survivors described a positive self-view, which was the most commonly reported benefit. Physical symptoms of the disease were the most commonly reported burden, reported by 32% of survivors (Straehla et al., 2017). In other studies, at the end of two years, a summary of quality-of-life scores using the SF-36 found that cancer survivors reported better scores than healthy controls (Jörngården et al., 2007; Larsson et al., 2010). Survivors of adolescent cancer reported higher scores on measurements of self-esteem, well-being, and expectations for the future than their peers in a healthy control group (Smorti, 2012).
In addition, changes in levels of depression, anxiety, and hope are significant predictors of changes in survivors’ quality of life (Germann et al., 2015). Increases in hope were found to partially mediate the effects of depression and anxiety on quality of life. In general, hope and quality of life improved as long as one year after diagnosis. However, 26% of participants reported symptoms of depression (Germann et al., 2015).
Types of Coping Strategies and Psychological Distress
Among adolescents, types of coping strategies differ based on time since diagnosis. The three types of coping strategies reported in this review were emotion-focused coping, problem-focused coping, and secondary control coping. Shortly after their cancer diagnoses, adolescents used all three coping strategies (Compas et al., 2014; Engvall et al., 2011; Enskär & von Essen, 2007; Hildenbrand et al., 2014; Kyngäs et al., 2001), and all were associated with lower psychological distress. A study by Hildenbrand et al. (2014) found that within two months of diagnosis, young adolescents used secondary control coping strategies, such as relaxing and seeking social support. In addition, participants reported thinking about, but rarely using, avoidant coping strategies (Hildenbrand et al., 2014).
Problem-focused coping: The coping strategy used most often by survivors of adolescent cancer was problem-focused coping, and those using this type of coping had psychological distress scores within normative ranges (Castellano-Tejedor et al., 2016). Most adolescents with cancer reported believing that they could manage their illness, and they used problem-focused coping strategies shortly after diagnosis (Engvall et al., 2011; Hildenbrand et al., 2014; Kyngäs et al., 2001; Turner-Sack et al., 2012). They also reported a desire for independence and sought information about cancer-related issues from books or the Internet (Kyngäs et al., 2001). In particular, information from parents, considered as problem-focused coping, was associated with better psychological outcomes (Castellano-Tejedor et al., 2016). In addition, adolescents with cancer who used problem-focused coping reported more post-traumatic growth (Turner-Sack et al., 2012).
Emotion-focused coping: Adolescents with cancer sought social support from family members or individuals who had also been diagnosed with cancer (Castellano-Tejedor et al., 2016; Enskär & von Essen, 2007; Kyngäs et al., 2001). Within two months of receiving a cancer diagnosis, adolescents often used accepting and minimizing thoughts as emotion-focused coping strategies to disrupt negative thought patterns. These strategies helped to alleviate stress (Engvall et al., 2011; Enskär & von Essen, 2007). Mothers’ positivity was a significant factor in newly diagnosed adolescents’ outlook on cancer diagnoses and treatment (Murphy et al., 2017).
Even five years after completion of cancer treatment, seeking social support was helpful in coping with difficulties related to cancer treatment and adapting to the school environment (Castellano-Tejedor et al., 2016; Kyngäs et al., 2001). Survivors who perceived high levels of emotional social support from friends, parents, and healthcare providers reported lower psychological distress and better adjustment in school (Castellano-Tejedor et al., 2016; Kyngäs et al., 2001). Adjustment in school is an important developmental task for adolescents, and social support helps survivors get back to the lives they had before diagnosis.
Avoidant coping: Within a few months of a cancer diagnosis, adolescents reported the use of avoidant coping strategies (e.g., avoidance, denial, disengagement, wishful thinking), which corresponded with higher levels of anxiety and depression (Compas et al., 2014). One year after a diagnosis of bone cancer, these adolescents continued to use more avoidant coping strategies than members of a healthy control group. They exhibited great impulse control in regulating these coping strategies, so their levels of psychological distress were within the normal range (Smorti, 2012).
Individuals with cancer use avoidant coping strategies more often than healthy peers (Castellano-Tejedor et al., 2016; Smorti, 2012). Avoidant coping strategies are associated with higher levels of psychological distress (Turner-Sack et al., 2012). The longer the time since cancer diagnosis (five years or more), the fewer the reports of avoidant coping strategies (Turner-Sack et al., 2012). This change in coping strategies may coincide with the idea that the potential for a return of the cancer drops after five years. At this point, survivors reported the use of problem-focused coping strategies most often (Castellano-Tejedor et al., 2016), followed by emotion-focused coping and secondary control strategies (Castellano-Tejedor et al., 2016; Turner-Sack et al., 2012).
However, survivors who used avoidant coping strategies (e.g., denial, drug abuse, a tendency to suppress negative thoughts) more than five years after diagnosis showed higher psychological distress (Turner-Sack et al., 2012; Wenninger et al., 2013). Avoidant coping was related to higher levels of anxiety and depression (Compas et al., 2014). However, because the studies with these findings did not use a longitudinal design, no causal relationship between the use of avoidant coping strategies and psychological distress could be determined.
Secondary control coping: Secondary control involves maximizing one’s coping based on the current situation, and the use of adaptive coping strategies is a significant predictor of decreased emotional distress (Compas et al., 2014). Shortly after a cancer diagnosis, secondary control coping strategies—acceptance or cognitive appraisal—helped to decrease symptoms of anxiety and depression (Compas et al., 2014). More than five years after completion of cancer treatment, the use of secondary control coping strategies helped to mediate negative thoughts about cancer treatment, promoted a higher concordance to medical regimens, and assisted in the management of stress (Wenninger et al., 2013). For example, how survivors of adolescent cancer felt about their diagnosis had a greater impact on their psychological distress than did their demographic or clinical characteristics. Coping strategies explained 38% of the variance in psychological distress, whereas demographic factors, such as gender, relationship status, and late medical effects, accounted for only 12% (Wenninger et al., 2013). Similarly, social support (e.g., informative and emotional support from parents, peers, and clinicians) and coping strategies explained about 30% of the psychosocial distress outcome model using a multiple regression analysis (Castellano-Tejedor et al., 2016).
Critique of Selected Studies
Some of the selected studies could be strengthened by using longitudinal designs that illustrate the coping and/or psychological distress process over time (Engvall et al., 2011; Enskär & von Essen, 2007; Germann et al., 2015; Jörngården et al., 2007; Larsson et al., 2010; Mattson et al., 2007; Murphy et al., 2017; Straehla et al., 2017; Wu et al., 2014). A few studies employed mixed methods that included objective data from questionnaires (Hildenbrand et al., 2014; Mattsson et al., 2007; Murphy et al., 2017). Using a mixed-methods approach combining quantitative and qualitative strategies could provide better understanding (Creswell & Clark, 2007) of how this population copes with cancer diagnosis and treatment. A study by Wu et al. (2014) used a randomized controlled design that provided the highest level of evidence supporting the results. Five studies included control groups, enabling the comparison of cancer survivors and healthy participants (Larsson et al., 2010; Maunsell et al., 2006; Michel et al., 2019; Smorti, 2012; Wu et al., 2014). Limitations of the selected studies are small sample size (Castellano-Tejedor et al., 2016; Enskär & von Essen, 2007; Jörngården et al., 2007; Murphy et al., 2017; Turner-Sack et al., 2012; Wu et al., 2014), self-selection bias (Michel et al., 2019; Murphy et al., 2017; Turner-Sack et al., 2012; Wenninger et al., 2013; Wu et al., 2014; Zamora et al., 2017), no report on the reliability of the instrument (Hildenbrand et al., 2014; Jörngården et al., 2007; Michel et al., 2019), no control group (Germann et al., 2015; Straehla et al., 2017), and outdated samples (Engvall et al., 2011; Maunsell et al., 2006). These limitations preclude a clear conclusion about how adolescents with cancer cope with cancer-related stress.
Discussion
Studies of survivors of adolescent cancer reveal that various forms of physical and psychological distress, including anxiety, depressive symptoms, and PTSD, are associated with cancer diagnosis and treatment. Adolescents who were older at the time of cancer diagnosis, were female, or had solid tumors that required surgery were more likely to experience high levels of psychological distress than others.
When adolescents were first diagnosed with cancer, more than half reported psychological distress at diagnosis. As time passed, the majority had levels of psychological distress equal to or lower than healthy controls (Jörngården et al., 2007; Larsson et al., 2010; Michel et al., 2019; Turner-Sack et al., 2012; Wenninger et al., 2013). In addition, most long-term survivors had good scores on health-related quality of life (Maunsell et al., 2006).
However, about one-sixth of survivors reported at least one type of psychological distress, such as anxiety and depression, more than five years later (Maunsell et al., 2006; Michel et al., 2019; Wenninger et al., 2013).
Problem- and emotion-focused coping strategies and secondary control coping strategies were reported as the most effective methods of reducing psychological distress (Hildenbrand et al., 2014; Kyngäs et al., 2001; Murphy et al., 2017; Smorti, 2012; Wenninger et al., 2013). Adolescents used different coping strategies depending on demographic- or illness-related characteristics. For example, those who were diagnosed during older adolescence used more primary control (problem- and emotion-focused) and avoidant coping strategies (Wenninger et al., 2013). The use of primary coping strategies might be related to their relatively advanced intellectual ability to understand abstract ideas and their ability to seek out needed information (Abrams et al., 2007). In a highly stressful environment, such as the acute phase of cancer treatment, avoidant coping strategies could help adolescents focus on tasks and not feel overwhelmed by emotions (Castellano-Tejedor et al., 2016; Wenninger et al., 2013). However, the use of avoidant coping strategies, such as thought suppression, after completion of treatment and over the years could create a risk for psychological distress. Wenninger et al. (2013) determined that allowing stress to go unresolved over a long period of time could put survivors of adolescent cancer at risk for increased psychological distress in later life. Studies found that thought suppression was associated with increased symptoms of PTSD (Wenninger et al., 2013).
Problem-focused and emotion-focused coping strategies were more effective over the life course and provided better outcomes (Maurice-Stam et al., 2009). Maurice-Stam et al. (2009) reported that young adult survivors of childhood cancer, who had positive expectations about their futures, reported higher scores on mental and physical quality-of-life surveys. Positive expectations for the future, optimism, and hope have been associated with positive mood, lower somatic distress, and better quality of life for survivors of adolescent cancer (Germann et al., 2015; Murphy et al., 2017; Smorti, 2012; Straehla et al., 2017). Healthcare providers, particularly nurses, are in a position to help these survivors learn effective coping strategies (Wenninger et al., 2013). Testing interventions that promote positive coping strategies is an important next step in helping those diagnosed with cancer during adolescence to have better psychological outcomes.
Social support from others is another coping strategy that provides better psychological outcomes (Lazarus & Folkman, 1984) and is most effective for adolescents in the first few months after diagnosis (Pennant et al., 2020). Pennant et al. (2020) determined that this social support from family, peers, and clinicians provides presence, distraction, and positivity, and facilitates communication and advocacy. In an integrative literature review, Decker (2007) reported that mothers are the major source of social support for adolescents with cancer. However, as children grow older, support from peers becomes more important (Enskär & von Essen, 2007). Shortly after a cancer diagnosis, adolescents experience considerable stress but also receive significant social support from family, friends, and healthcare providers (Enskär & von Essen, 2007; Hildenbrand et al., 2014; Kyngäs et al., 2001). After completion of cancer treatment, adolescents needed information and advice from healthcare providers, but had fewer appointments with healthcare providers compared to the period when they were undergoing treatment (D’Agostino et al., 2011). Some turned to family and friends for emotional social support (Castellano-Tejedor et al., 2016), which served as a buffer against unresolved psychological distress.
The use of adaptive coping strategies, such as problem- or emotion-focused coping, discouraged psychological distress and encouraged post-traumatic growth among survivors (Mattsson et al., 2007; Turner-Sack et al., 2012). An individual who experiences a traumatic event such as cancer may experience emotional and mental growth beyond that of their peers (Zamora et al., 2017). Two years after diagnosis, survivors of adolescent cancer reported positive and negative effects from cancer diagnosis and treatment (Mattsson et al., 2007). Negative effects included unpleasant thoughts, feelings of isolation, and difficulty concentrating on schoolwork (Mattsson et al., 2007). However, survivors concluded that there were more benefits than burdens at this point in their lives. They reported a shift in perspective over time and a positive view of self and their futures (Straehla et al., 2017).
The use of secondary control coping strategies was also helpful in decreasing psychological distress from shortly after cancer diagnosis through completion of treatment (Compas et al., 2014; Wenninger et al., 2013). Consequently, encouraging the use of secondary control coping strategies could be an effective tool for survivors after a cancer diagnosis and over the life course (Compas et al., 2014). A study by Compas et al. (2012) has shown that children and adolescents can learn secondary control coping skills through cognitive behavioral interventions. In another study, Wu et al. (2014) used a psychoeducational intervention to increase coping strategies and decrease symptom severity in survivors two years after diagnosis. Although there were no differences in coping scores between the intervention and control groups, the intervention group reported that most symptoms, including pain, psychoneurologic problems, and negative body image, significantly decreased over time compared to the control group.
As time passes after a diagnosis of cancer, survivors tended to focus less on the physical aspects of the disease and treatment and more on their personal strengths and purpose in life (Straehla et al., 2017). Prati & Pietrantoni (2009), using a meta-analysis, found that emotion-focused coping strategies and secondary control coping strategies, such as acceptance, were strongly correlated with post-traumatic growth. Post-traumatic growth, in turn, was associated with better physical and mental health (Arpawong et al., 2013). Interviewed 20 years after a cancer diagnosis, some survivors continued to report this positive outlook and specifics about increased personal growth, improved relationships with others, new possibilities, an appreciation for life, and spiritual development (Zamora et al., 2017).
Limitations
The aims of this research were to understand the relationship between coping strategies and psychological distress and to examine factors that affect cancer survivors’ abilities to cope over time. Various age groups are represented in the studies selected for inclusion in this review. Some survivors were still adolescents, whereas others were middle-aged, at the time of data collection. This might affect the interpretation of coping strategies between more recently diagnosed survivors and those diagnosed in the more distant past. In addition, most of the studies reviewed were conducted in the United States, prohibiting the generalization of findings. Exploration of possible cultural differences in psychological distress and coping among survivors, their families, and clinicians was not possible. The authors of the selected articles used several different instruments to measure coping strategies, which limited the current authors’ ability to compare findings.
Implications for Practice
Healthcare providers, particularly nurses, need to regularly assess survivors’ negative thoughts or feelings and be aware of early symptoms of psychological distress. In this review, three types of coping strategies were considered effective in decreasing psychological distress: problem-focused coping, emotion-focused coping, and secondary control coping. More longitudinal studies and those with a larger sample are needed to confirm a pattern of psychological adjustment and coping strategies in adolescents dealing with cancer diagnosis and/or treatment. Understanding this process is necessary as a step toward development of evidence-based interventions. Also, future research might focus on cancer survivors who were initially diagnosed with cancer during adolescence and their coping strategies in subsequent years. Future research might seek to develop patient categories that could be used to predict which individuals would most benefit from which coping strategies. In turn, this would enable healthcare providers to tailor their teaching of coping strategies to individual patients. Another potential area for exploration is the measurement of change in psychological distress and coping strategies over time to develop best practices in care and ensure optimal patient outcomes.
In addition, there are promising interventions that may well serve the adolescent cancer survivor population. Some researchers are using telephone-based interventions as well as psychoeducational programs in care plans for adolescents with cancer (Santacroce et al., 2010). A web-based intervention program has been shown to help adolescents with cancer seek information for themselves (O’Conner-Von, 2009). These web- and telephone-based interventions take into account various characteristics of adolescents: the desire to have information, the appeal of anonymity versus in-person meetings, and the need to learn independently. It is important to further examine the potential benefits of these technologies for adolescent cancer survivors to improve clinical practices and health outcomes. 
Conclusion
Cancer diagnosis and treatment during adolescence adds physical difficulties and psychological distress to the disease state. This population’s unique needs should be considered when designing and testing interventions. This review of 19 studies reveals important findings about the types of coping strategies used by adolescent cancer survivors. Adolescents reported varying degrees of psychological distress, affected by a host of disease and environmental factors. Most of them improved significantly over time and were able to regain a positive outlook on their futures. More research is necessary to reveal which coping strategies—problem-focused coping, emotion-focused coping, and secondary control coping—are most effective for adolescents at which stages in the disease process. Immediately following a diagnosis, adolescent cancer survivors could benefit from tailored interventions aimed at teaching them effective coping strategies based on their specific diagnosis, age, and time since diagnosis. These strategies have the potential to help patients maintain optimal levels of psychological health, important for their overall health and well-being, in recovery and beyond.
About the Author(s)
Hyewon Shin, RN, PhD, is an assistant professor in the School of Nursing at Clemson University in Greenville, SC; Robin Bartlett, RN, PhD, is a professor and lifespan researcher in the Capstone College of Nursing at the University of Alabama in Tuscaloosa; and Jennie C. De Gagne, PhD, DNP, RN, NPD-BC, CNE, ANEF, FAAN, is an associate professor in the School of Nursing at Duke University in Durham, NC. No financial relationships to disclose. Shin and De Gagne contributed to the conceptualization and design. Shin completed the data collection. All authors provided the analysis and contributed to the manuscript preparation. Shin can be reached at shin@clemson.edu, with copy to ONFEditor@ons.org. (Submitted April 2019. Accepted March 9, 2020.)